

COPD includes Asthma,Bronchitis, especially Emphysema!
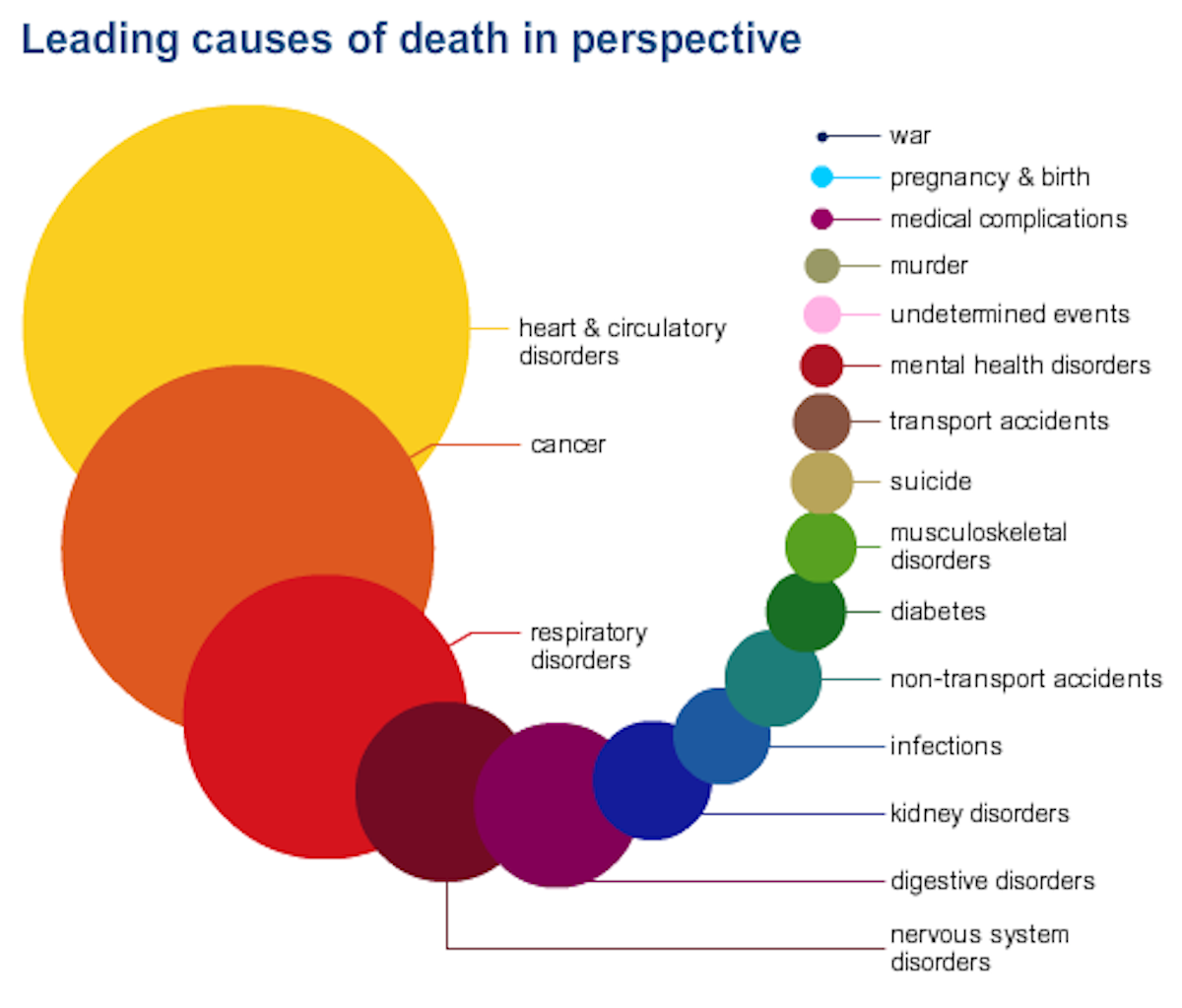
2: Cancer (malignant neoplasms)
- Deaths: 576,691
- Males: 302,231
- Females: 274,460
- Rate: 185.1
- Age-adjusted rate: 169.0
- Percentage of total deaths: 22.92%.
Cancer affects men and woman of all ages, races and ethnicities.5 The National Institutes of Health (NIH) estimate the total costs of cancer in 2009 were $216.6 billion: $86.6 billion for direct medical costs and $130.0 billion for indirect mortality costs.
Cancer is a group of diseases characterized by the uncontrolled growth and spread of abnormal cells. If the spread is not controlled, it can result in death.
In 2014, about 585,720 American are expected to die of cancer – almost 1,600 people per day.
Lung cancer accounts for more deaths than any other cancer in both men and women. Deaths from cancer of the trachea, bronchus and lung stand at 157,017 annually with this figure expected to rise to 159,260 in 2014.
Estimated cancer-related deaths for 2014
Leading causes of death from cancer for males:
- Lung and bronchus – 86,930 (28%)
- Prostate – 29,480 (10%)
- Colon and rectum – 26,270 (8%)
- Pancreas – 20,170 (7%)
- Liver and intrahepatic bile duct – 15,870 (5%)
- Leukemia – 14,040 (5%)
- Esophagus – 12,450 (4%)
- Urinary bladder – 11,170 (4%)
- Non-Hodgkin lymphoma – 10,470 (3%)
- Kidney and renal pelvis – 8,900 (3%).
Leading causes of death from cancer for females:
- Lung and bronchus – 72,330 (26%)
- Breast – 40,000 (15%)
- Colon and rectum – 24,040 (9%)
- Pancreas – 19,420 (7%)
- Ovary – 14,270 (5%)
- Leukemia – 10,050 (4%)
- Uterine corpus – 8,590 (3%)
- Non-Hodgkin lymphoma – 8,520 (3%)
- Liver and intrahepatic bile duct – 7,130 (3%)
- Brain and other nervous system – 6,230 (2%).
Can cancer be prevented?
A substantial proportion of cancers could be prevented. All cancers caused by cigarette smoking and heavy use of alcohol could be prevented completely. In 2014, almost 176,000 of the estimated 585,720 deaths will be caused by tobacco use.
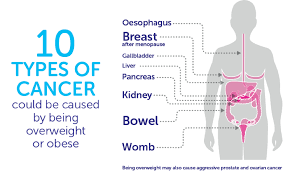
The World Cancer Research Fund has estimated that up to one-third of cancer cases that occur in economically developed countries like the US are related to being overweight, obese, inactive or having poor nutrition. These are all potentially preventable.
Particular cancers are related to infectious agents such as human papillomavirus (HPV), hepatitis B virus (HBV), hepatitis C virus (HCV), human immunodeficiency virus (HIV) and helicobacter pylori (H. pylori) – these may be prevented through behavioral changes and use of protective vaccinations or antibiotic treatments.
Many of the more than 3 million skin cancer cases that are diagnosed annually could be prevented by protecting skin from excessive sun exposure and avoiding indoor tanning.
Screening offers the ability for secondary prevention by detecting cancer early, before symptoms appear. Early detection usually results in less extensive treatment and better outcomes.
Screening for colorectal and cervical cancers can prevent cancer by allowing for detection and removal of pre-cancerous lesions.
Awareness about changes in the body to breasts, skin or testicles may result in detection of tumors at an earlier stage.
Learn more about cancer at the American Cancer Society or Caner treatment.com with so many other places on the internet, to our library, to our MD and much more. All you have to do is research, take the time.
3: Chronic lower respiratory disease
- Deaths: 142,943
- Males: 67,521
- Females: 75,422
- Rate: 45.9
- Age-adjusted rate: 42.5
- Percentage of total deaths: 5.68%.
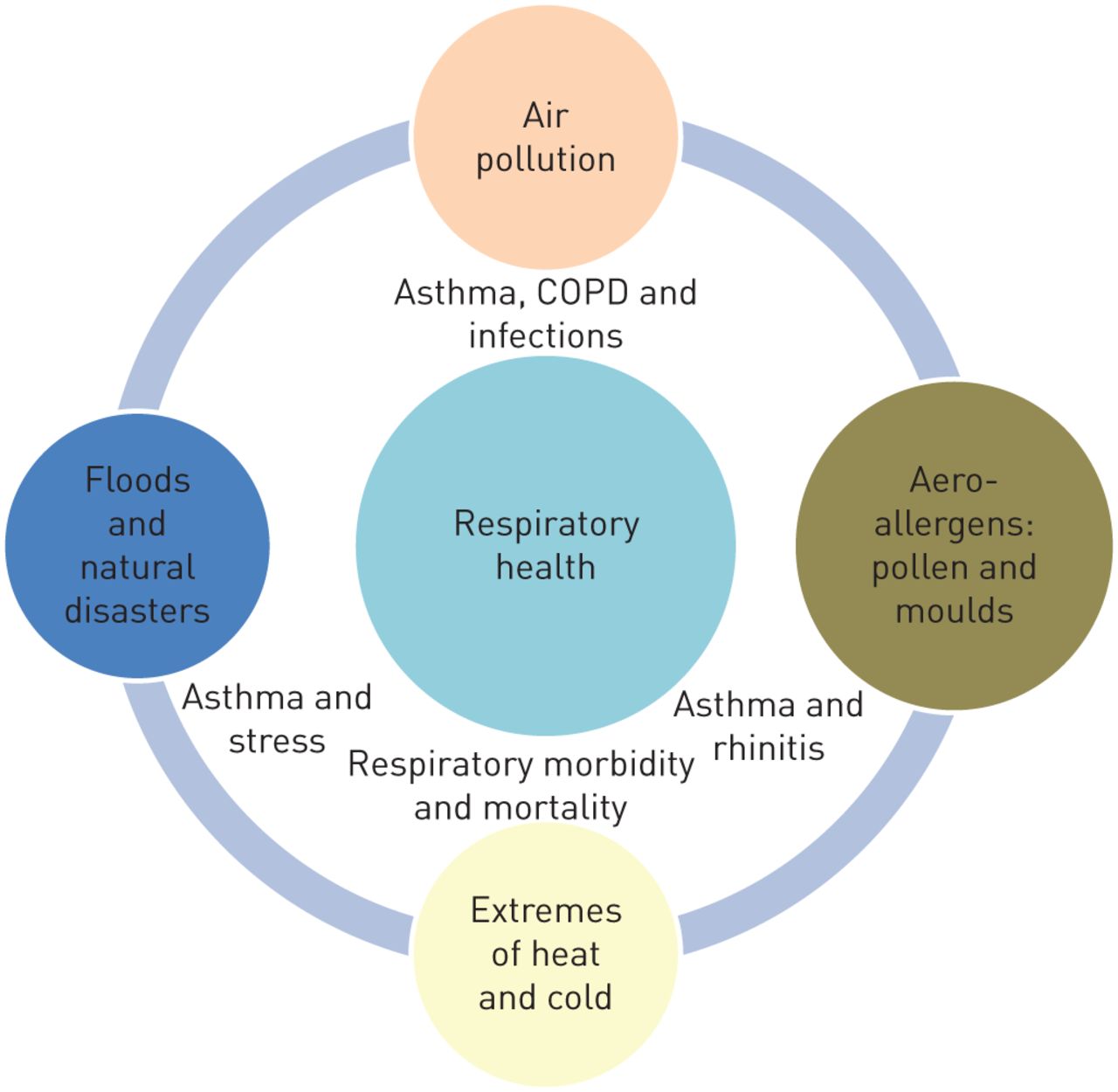
Chronic lower respiratory disease (CLRD) is a collection of lung diseases that cause airflow blockage and breathing-related issues, including primarily chronic obstructive pulmonary disease (COPD) but also bronchitis, emphysema (is due to alot of smokers) and asthma.
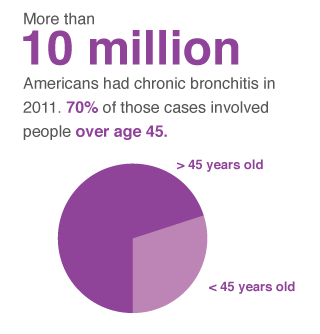
Bronchitis (chronic) has active and inactive stages where most get it through their lifetime. How often has depending factors. Bronchitis may be either acute or chronic. Often developing from a cold or other respiratory infection, acute bronchitis is very common.
*Chronic bronchitis, a more serious condition, is a constant irritation or inflammation of the lining of the bronchial tubes, often due to smoking.
*Acute bronchitis usually improves within a few days without lasting effects, although you may continue to cough for weeks. However, if you have repeated bouts of bronchitis, you may have chronic bronchitis, which requires medical attention.
A study released by The American College of Chest Physicians (CHEST) estimated that 16.4 million days of work were lost annually because of COPD, and total absenteeism costs were $3.9 billion. Of the medical costs, 18% was paid for by private insurance, 51% by Medicare, and 25% by Medicaid. National medical costs are projected to increase from $32.1 billion in 2010 to $49.0 billion in 2020.8,9
Major warning signs and symptoms of COPD
Signs and symptoms of COPD may include:
- Increased breathlessness when active
- A persistent cough with phlegm
- Frequent chest infections.
How can COPD be prevented?
In the US, tobacco smoke is a KEY FACTOR in the development and progression of COPD=EMPHYSEMA, although exposure to air pollutants in the home and workplace, genetic factors, and respiratory infections also play a role.7
Smoking is a primary risk factor of COPD since it causes primarily emphysema, and approximately 80% of COPD deaths can be attributed to smoking. Emphysema damages the tissue of the lung called alveoli causing them to expand and not have the elasticity they need to exchange 0xygen for carbon dioxide when we breath. Most importantly when the alveoli looses the elasticity it can’t be fixed unless you need a new lung and are a candidate for one. So regular daily smokers why don’t you just drink poison? Best is to not smoke at all but at least do it once in a awhile. Abusing anything usually turns into injury (For example take alcohol to simply verbally or physically abusing and doing it over and over again which makes it easier to do which isn’t right to do at all. Abuse is just used as an exampte not that it is right at all, I reenforce)
To prevent COPD:
- Quit smoking
- Avoid secondhand smoke
- Avoid air pollution
- Avoid chemical fumes
- Avoid dust
The FDA have approved the once-daily inhaled drug olodaterol (brand name Striverdi Respimat), a long-acting beta-agonist, for the treatment of airflow obstruction in COPD patients.
Doctors are missing chances to diagnose COPD early in up to 85% of cases
COPD is a progressive disease that causes irreversible damage to the lungs. Now, a new study reveals that doctors are missing chances to diagnose the condition early.
If this correct than that gives us as people not to depend just on the MD but to take care of ourselves in particular on preventative measures to give you higher odds that you will not even have to deal with the diagnosis at all.