“The 10th leading cause in America is Suicide. Each year 44,965 Americans die by suicide. Know for every suicide 25 attempts. Suicide costs the US $ 69 Billion annually.”
American Foundation for Suicide Prevention
“The 10th leading cause in America is Suicide. Each year 44,965 Americans die by suicide. Know for every suicide 25 attempts. Suicide costs the US $ 69 Billion annually.”
American Foundation for Suicide Prevention
“Sigmund Freud used to refer to depression as anger turned inward. While many people may regard this as an overly simplistic approach to the most common mental health disorder in the world, there is no doubt that anger plays a significant role in depression.”
“Dog lovers know how much warmth and comfort their canine companions add to their lives. But they might not know that a growing body of evidence suggests that having a dog may help improve heart health.”
Harvard Medical School – Harvard Health Publishing (www.health.harvard.edu)
“When kidneys fail, your body may have difficulty filtering your blood and keeping your body chemically balanced. Dialysis is a treatment process that cleans the body of unwanted toxins, waste products and excess fluids.”
Fresenius Kidney Care (freseniuskidneycare.com)
” “Transplant tourists” are traveling to established destinations to obtain readily accessible organs for transplantation, available from the poor of that destination country who sell mostly kidneys, but in some instances, a lobe of the liver or a cornea. These practices have been well known for more than a decade.”

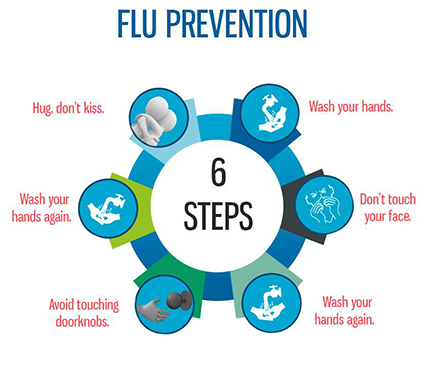
“Whether you’re ready or not, cold and flu season is right around the corner. But fortunately, you don’t have to settle for the inevitable. With a small amount of preparation and prevention, you can be ready. There are no guarantees when it comes to colds and the flu. The vaccine for the flu is great for prevention.”
Inter-mountain Healthcare




Winter is now around, so is the flu! While many people look forward to the cold weather for skiing and other outdoor activities, others heads have gone indoors until spring, cutting down on their opportunities for the exercise they need. Staying indoors with someone who has the flu you keep inhaling that air which will prone you in getting the flu as opposed to getting outside. Remember in a hospital your put on Droplet precaution, in a isolated room and droplet means you can catch the Flu within arm’s length of the pt; so you wear a mask when visiting the patient with the flu in a hospital.
So get outside in warmer or when the temp gets colder. Whether it’s spending an afternoon at the local sled hill with the kids or skiing down the Alps, you can help your clients and patients – not to mention yourself – maintain an active lifestyle in the wintertime while it still lasts.
Shoveling snow, building a snowman or going on a deep-snow hike all increase a person’s heart rate, oxygen consumption and energy expenditure. Skiing, snowboarding or ice skating strengthen the musculoskeletal system and improve balance and skill. Cross-country skiing, with its whole-body challenge, improves cardiovascular fitness and muscular endurance. And all winter sports connect us with the elements: wind, snow and, for some, the sublime beauty of the mountains.
Participating in winter activities may increase energy and fluid needs, especially if the person is engaging in vigorous and demanding activities. High altitude and cold temperatures can also increase energy expenditures — as much as two- or three-fold if you’re shivering. With winter activities, it is easy to forget to stay hydrated and fueled all day, so it’s imperative to take breaks to fuel up.
Exercising in the cold and at altitude exacerbates fluid loss in the body. A significant amount of fluid is lost through increased respiration and the body’s need to humidify dry, cold mountain air. In addition, cold-induced diuresis will lead to increased urinary volume and fluid loss. And cold reduces the body’s thirst response, making it a challenge to maintain fluid balance in the cold. However, dehydration in the cold has serious consequences; it impairs thermo-regulation and increases the risk of hypothermia.
With this in mind, it is best to begin exercise well-hydrated with water breaks (3 to 8 ounces) every 15 to 20 minutes if going out on the slopes for less than 60 minutes. For any time longer than an hour, consider recommending a sports beverage.
Altitude may increase the body’s need for vitamins and minerals. Adequate iron stores are necessary to increase red cell mass if exposure to altitude occurs on a regular basis. In other words, iron depletion interferes with the positive adaptation of the blood’s oxygen carrying capacity that typically occurs in response to exercise at altitude. Furthermore, altitude exposure increases the generation of reactive oxygen species. However, it remains debatable whether antioxidants such as vitamin E and C are needed in higher amounts to protect cells from damage when participating in exercise at altitude.
This topic is largely understudied in winter sports, and may be more concerning for elite athletes training at altitude. A balanced diet including a hearty vegetable soup with herbs and spices, a handful of nuts, an orange and a cup of green tea may be plenty to protect the cells from occasional winter outings.
Engaging in any type of cold-weather sports, especially at higher elevations, requires appropriate preparation in terms of clothing, shelter and the foods and fluids a person consumes before, during and after the activity. Recommend that your clients and patients take breaks throughout the day and listen to their bodies to ensure that they are feeling well and ready for another round of winter activity. Staying active outside can possibly help with keeping the Flu away especially if your exposed to someone in the house with the flu your not breathing the same air in the house which will prone you to getting the flu as opposed to staying active outdoors. Best thing in prevention of the flu is the vaccine but always check with your doctor.
“The number one thing you can do to prevent the flu is get vaccinated,” says Bill Schaffner, M.D., a professor of preventive medicine at Vanderbilt University. Even if another strain infects you, the shot may reduce symptoms.
Today (www.today.com)
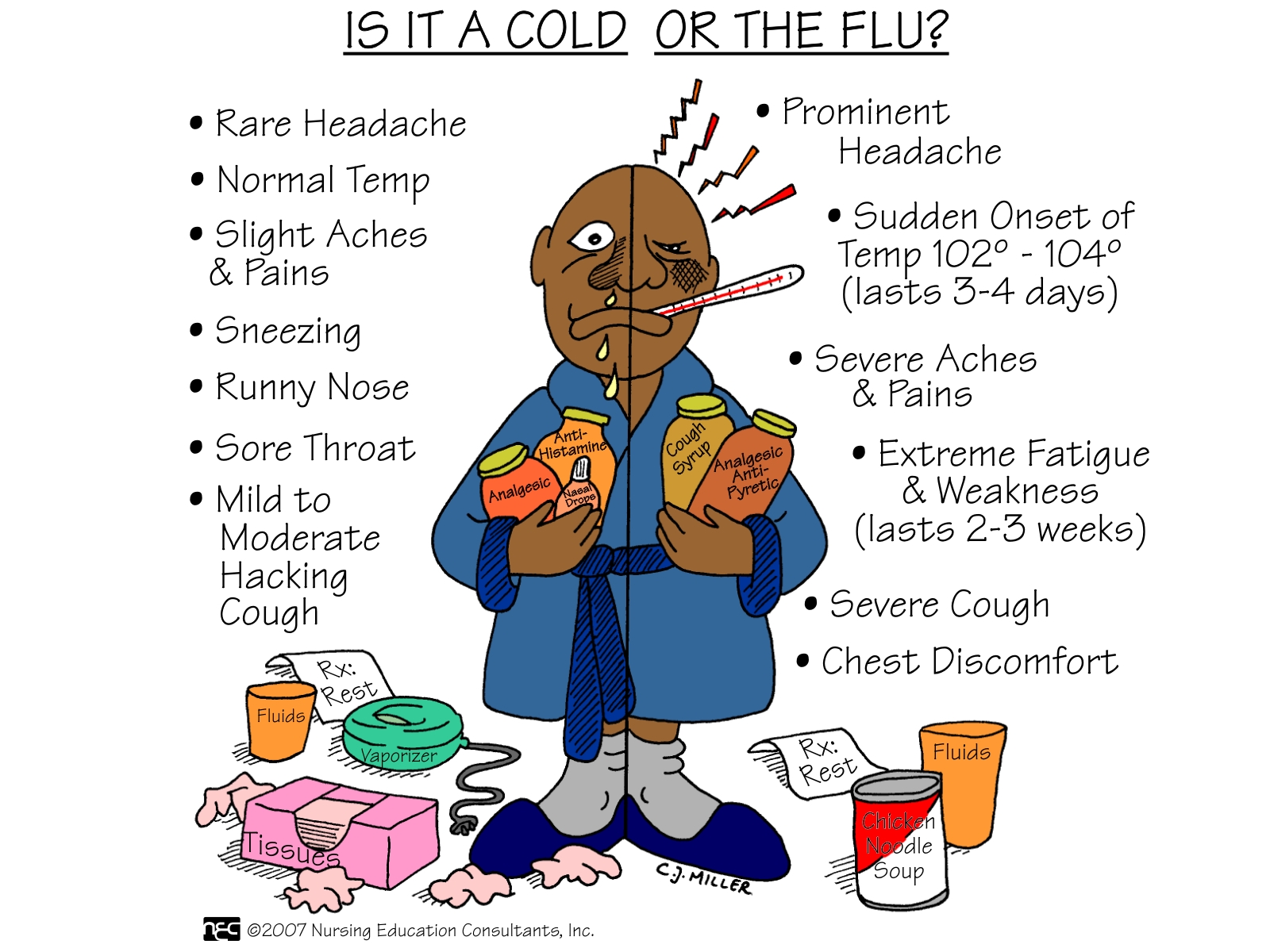
FLU FACTS:
-Both colds and flu usually last the same seven to 10 days, but flu can go three to four weeks; the flu virus may not still be there, but you have symptoms long after it has left. Allergy can last weeks or months.
-The winter flu epidemic will be coming around us again and in a given locality it reaches its peak in 2 to 3 weeks and lasts 5 to 6 weeks. Then is disappears as quickly as it arrived. The reason for this is not completely clear. The usual pattern is for a rise in the incidence of flu in children, which precedes an increase in the adult population.
-The flu virus can lead to serious complications, including bronchitis, viral or bacterial pneumonia and even death in elderly and chronically ill patients. Twenty thousand or more people die of the flu in the America each year. Know this that the frequency of human contact across the world and the highly infectious nature of the virus make this explanation difficult to accept. Moreover there is no evidence of persistent or latent infection with influenza viruses. In any case, this idea is not really very difficult from the notion that the virus circulates at a low level throughout the year and seizes its opportunity to cause an outbreak when conditions allow.
-Even harder to explain is why the flu disappears from a community when there are still a large number of people susceptible to infection. Than even harder than that is why flu is a winter disease, which is not fully understood or known. However, flu is spread largely by droplet (aerosol) infection from individuals with high viral level in their nasal and throat secretions, sneezing, and coughing on anyone close at hand. The aerosol droplets of the right size (thought to be about 1.5 micrometers in diameter) remain airborne and are breathed into the nose or lungs of the next victim.
-Situations in which people are crowded together are more commonly in cold or wet weather and so perhaps this contributes to spreading the flu at these times. It is interesting that in equatorial countries, flu occurs throughout the year, but is highest in the monsoon or rainy season. Enough about facts but onto logical thinking for when we or someone we know has it and what questions we might be asking ourselves.