“Legionnaires’ disease usually develops two to 10 days after exposure to legionella bacteria. It frequently begins with the following signs and symptoms: Headache, Muscle Aches, Fever that may be 104 F (40 C) or higher.”.
MAYO CLINIC
“Legionnaires’ disease usually develops two to 10 days after exposure to legionella bacteria. It frequently begins with the following signs and symptoms: Headache, Muscle Aches, Fever that may be 104 F (40 C) or higher.”.
MAYO CLINIC
“Legionnaires’ disease and Pontiac Fever are collectively known as Legionellosis, a disease caused by Legionella bacteria. Managing Legionella and preventing worker exposures and Legionellosis cases depend on implementing an effective water management program. These programs focus on describing water systems and their components, identifying areas where Legionella could grow, deciding where control measures are needed and how to monitor them, planning response actions when control measures fail, and monitoring and documenting water management activities.”.
United States Department of Labor (OSHA Occupational Health and Administration).
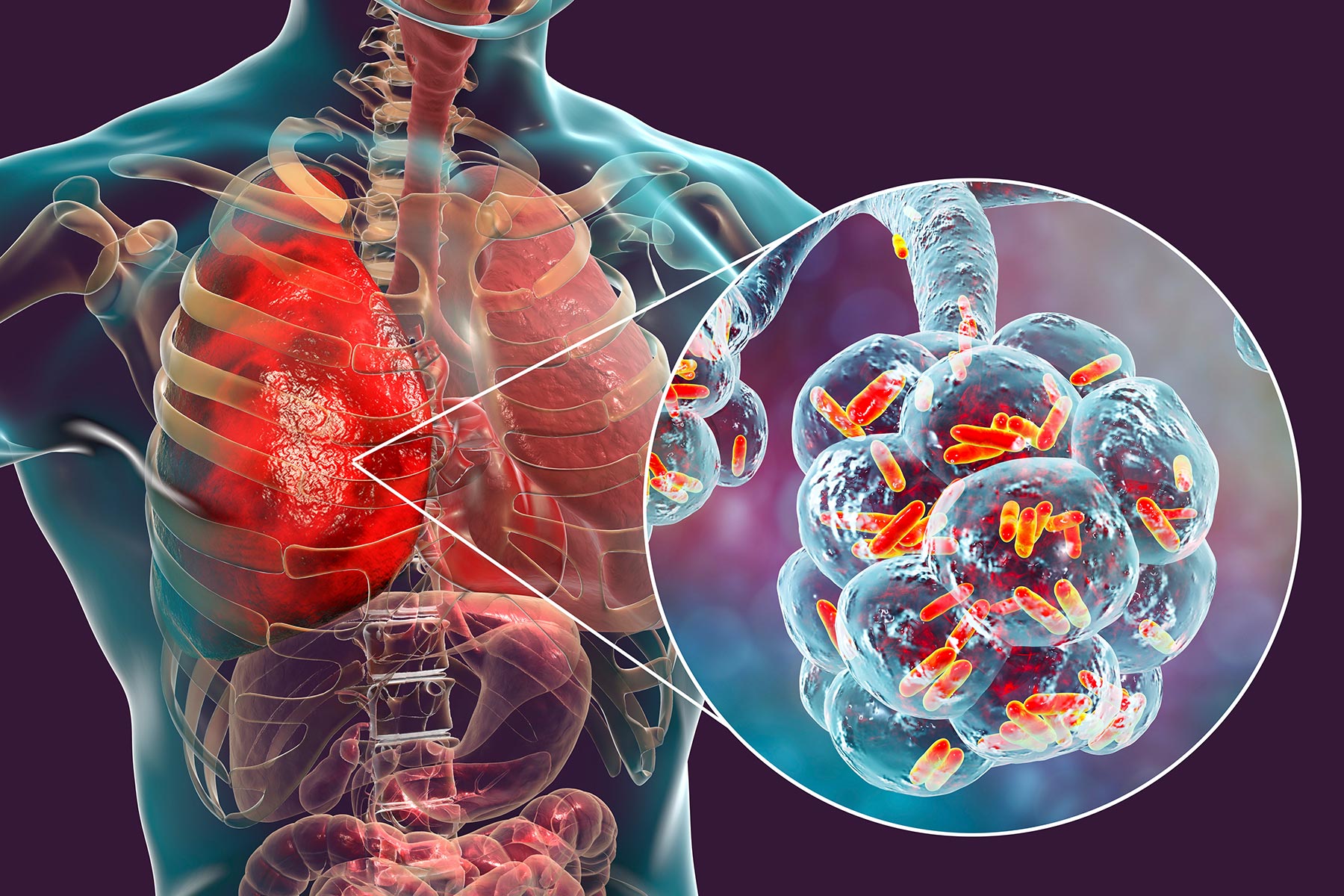
“Legionella bacteria can cause a serious type of pneumonia (lung infection) called Legionnaires’ disease. Legionella bacteria can also cause a less serious illness called Pontiac fever. Legionella bacteria are found naturally in freshwater environments, like lakes and streams. The bacteria can become a health concern when they grow and spread in human-made building water systems.”.
Centers for Disease Control and Prevention (CDC)
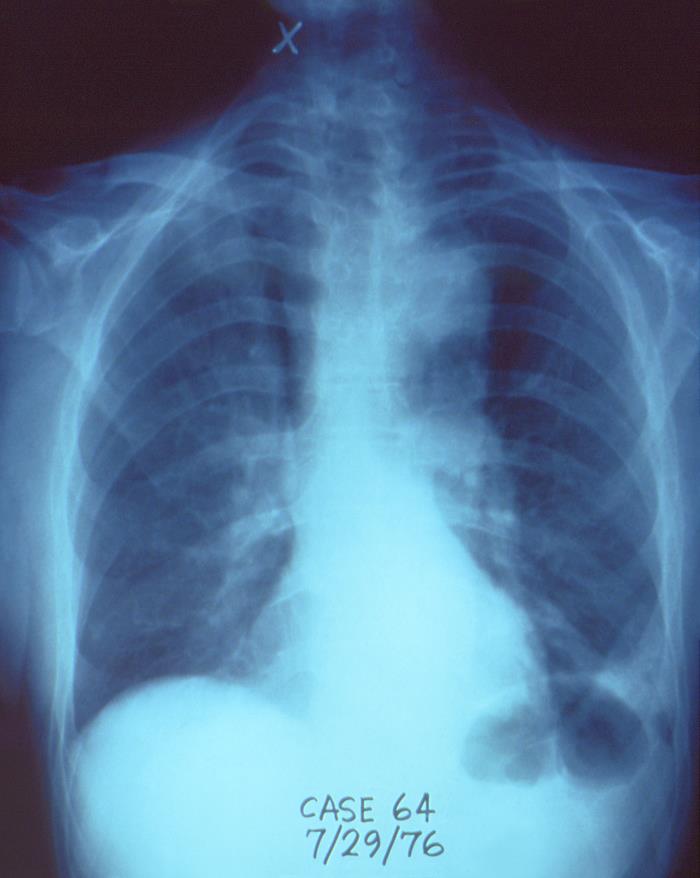

Legionella was discovered after an outbreak in 1976 among people who went to a Philadelphia convention of the American Legion. Those who were affected suffered from a type of pneumonia that eventually became known as Legionnaires’ disease.
The first identified cases of Pontiac fever occurred in 1968 in Pontiac, Michigan, among people who worked at and visited the city’s health department. It wasn’t until Legionella was discovered after the 1976 Legionnaires’ disease outbreak in Philadelphia that public health officials were able to show that Legionella causes both diseases.
Legionella bacteria are found naturally in freshwater environments, like lakes and streams. The bacteria can become a health concern when they grow and spread in human-made building water systems like
Home and car air-conditioning units do not use water to cool the air, so they are not a risk for Legionella growth.
However, Legionella can grow in the windshield wiper fluid tank of a vehicle (such as a car, truck, van, school bus, or taxi), particularly if the tank is filled with water and not genuine windshield cleaner fluid.
After Legionella grows and multiplies in a building water system, water containing Legionella can spread in droplets small enough for people to breathe in. People can get Legionnaires’ disease or Pontiac fever when they breathe in small droplets of water in the air that contain the bacteria.
Less commonly, people can get sick by aspiration of drinking water containing Legionella. This happens when water accidently goes into the lungs while drinking. People at increased risk of aspiration include those with swallowing difficulties.
In general, people do not spread Legionnaires’ disease and Pontiac fever to other people. However, this may be possible under rare circumstances.
“Cholera is an acute diarrhoeal infection caused by ingestion of food or water contaminated with the bacterium Vibrio cholerae. Cholera remains a global threat to public health and an indicator of inequity and lack of social development.”
World Health Organization (WHO)
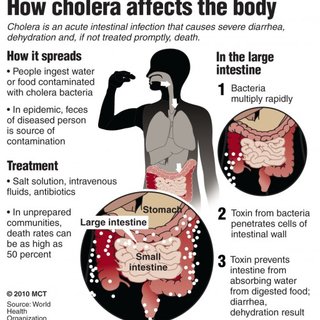

Cholera is an acute diarrheal illness caused by infection of the intestine with Vibrio cholerae bacteria. People can get sick when they swallow food or water contaminated with cholera bacteria. The infection is often mild or without symptoms, but can sometimes be severe and life-threatening.
About 1 in 10 people with cholera will experience severe symptoms, which, in the early stages, include:
Cholera has been nicknamed the “blue death” because a person’s skin may turn bluish-gray from extreme loss of fluids. As dehydration racks the body, blood would begin to thicken in patients’ veins; starved of oxygen, the skin would turns sickly shade of blue. Lack of oxygen for over a several minutes can cause blue of the skin.
Cholera is treated with hydration (given either orally or intravenously), electrolytes, and antibiotics.
The word cholera is from Greek: χολέρα kholera from χολή kholē “bile”. Cholera likely has its origins in the Indian subcontinent as evidenced by its prevalence in the region for centuries.
The disease appears in the European literature as early as 1642, from the Dutch physician Jakob de Bondt’s description it in his De Medicina Indorum. (The “Indorum” of the title refers to the East Indies. He also gave first European descriptions of other diseases.) .
Early outbreaks in the Indian subcontinent are believed to have been the result of poor living conditions as well as the presence of pools of still water, both of which provide ideal conditions for cholera to thrive. The disease first spread by trade routes (land and sea) to Russia in 1817, later to the rest of Europe, and from Europe to North America and the rest of the world, (hence the name “Asiatic cholera”). Seven cholera pandemics have occurred in the past 200 years, with the seventh pandemic originating in Indonesia in 1961.
The first cholera pandemic occurred in the Bengal region of India, near Calcutta starting in 1817 through 1824. The disease dispersed from India to Southeast Asia, the Middle East, Europe, and Eastern Africa. ***The movement of British Army and Navy ships and personnel is believed to have contributed to the range of the pandemic, since the ships carried people with the disease to the shores of the Indian Ocean, from Africa to Indonesia, and north to China and Japan.***
The second pandemic lasted from 1826 to 1837 and particularly affected North America and Europe due to the result of advancements in transportation and global trade, and increased human migration, including soldiers.
The third pandemic erupted in 1846, persisted until 1860, extended to North Africa, and reached South America, for the first time specifically affecting Brazil.
The fourth pandemic lasted from 1863 to 1875 spread from India to Naples and Spain.
The fifth pandemic was from 1881–1896 and started in India and spread to Europe, Asia, and South America.
The sixth pandemic started 1899–1923. These epidemics were less fatal due to a greater understanding of the cholera bacteria. Egypt, the Arabian peninsula, Persia, India, and the Philippines were hit hardest during these epidemics, while other areas, like Germany in 1892 (primarily the city of Hamburg where more than 8.600 people died) and Naples from 1910–1911, also experienced severe outbreaks.
The seventh pandemic originated in 1961 in Indonesia and is marked by the emergence of a new strain, nicknamed El Tor, which still persists (as of 2018) in developing countries.
Cholera became widespread in the 19th century. Now Cholera cases are much less frequent in developed countries where governments have helped to establish water sanitation practices and effective medical treatments.
Cholera morbus is a historical term that was used to refer to gastroenteritis rather than specifically cholera. You’re most likely to get viral gastroenteritis when you eat or drink contaminated food or water. You may also be likely to get gastroenteritis if you share utensils, towels or food with someone who has one of the viruses that cause the condition. Many viruses can cause gastroenteritis, including: Noroviruses.
“Heart disease is the leading cause of death for men, women, and people of most racial and ethnic groups in the United States. One person dies every 36 seconds in the United States from cardiovascular disease. About 659,000 people in the United States die from heart disease each year—that’s 1 in every 4 deaths. Heart disease costs the United States about $363 billion each year from 2016 to 2017.2 This includes the cost of health care services, medicines, and lost productivity due to death.”
Centers for Disease Control and Prevention (CDC)
“Leber congenital amaurosis (LCA) is a rare type of inherited eye disorder that causes severe vision loss at birth. It is the most common cause of inherited blindness in childhood, and is found in two to three out of every 100,000 babies. The retina has two main types of cells: cones and rods. Cone and rod cells are called photoreceptors because they detect and respond to light stimuli. LCA affects both the peripheral rod cells, which allow you to see at night, and the central cone cells, responsible for fine detail and color vision.
LCA is inherited in an autosomal recessive manner, meaning that both parents must carry a defective gene for the condition in order to pass it on to their children. Each of their children has a 25 percent chance of inheriting the two LCA genes (one from each parent) needed to cause the disorder.”
University of California San Francisco UCSF


Leber congenital amaurosis (LCA) is an eye disorder that primarily affects the retina. LCA is most typically passed through families by the autosomal recessive pattern of inheritance. In this type of inheritance, both parents, called carriers, have one gene for the disease paired with one normal gene. Each of their children has a 25 percent chance (or 1 chance in 4) of inheriting the two LCA genes (one from each parent) needed to cause the disorder. Carriers are unaffected because they have only one copy of the gene. At this time, it is impossible to determine who is a carrier for LCA until after the birth of an affected child.People with this condition typically have severe visual impairment beginning in infancy.
Signs or symptoms with this disease include:
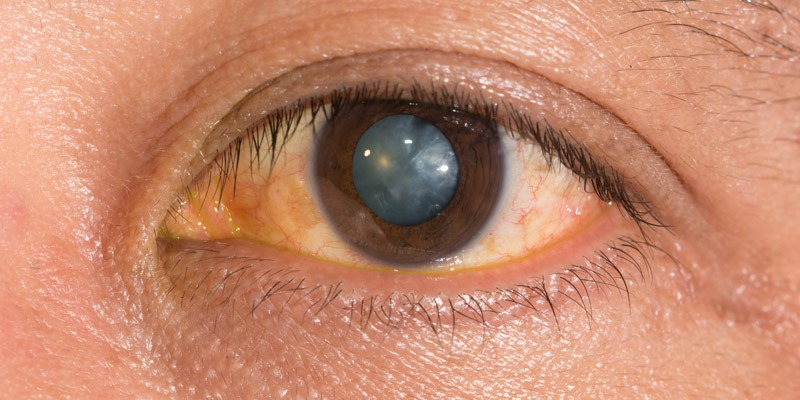
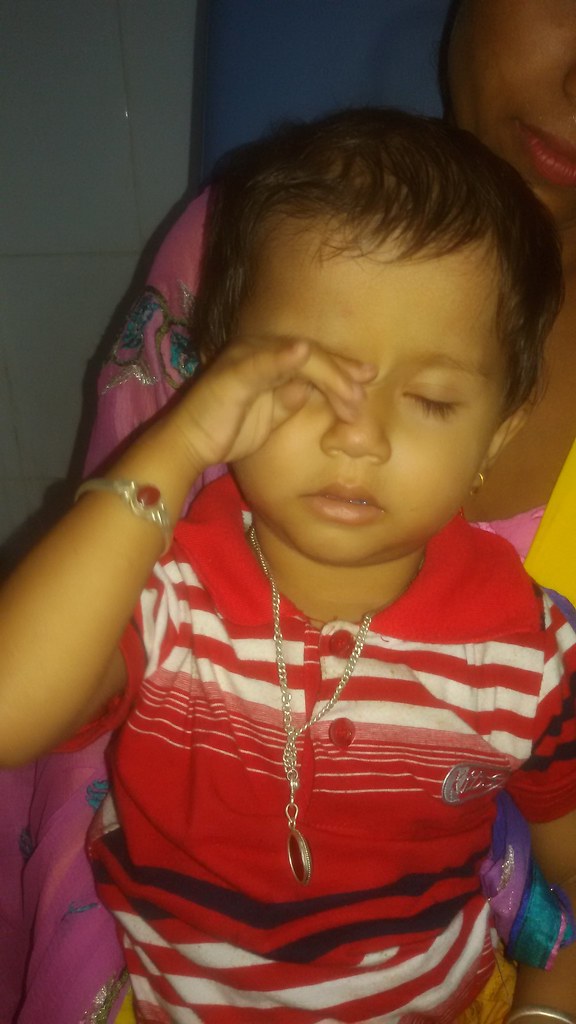
Photophobia, involuntary movements of the eyes (nystagmus), and extreme farsightedness. The pupils also do not react normally to light. Additionally, the cornea may be cone-shaped and abnormally thin (keratoconus). Franceschetti’s oculo-digital sign is characteristic of Leber congenital amaurosis. This sign consists of poking, pressing, and rubbing the eyes with a knuckle or finger. Different subtypes have been described. The different subtypes are caused by genetic changes in different genes. Some of these subtypes are also distinguished by their patterns of vision loss and related eye abnormalities.
Leber congenital amaurosis (LCA) is a rare genetic eye disorder. Affected infants are often blind at birth. Other symptoms may include crossed eyes (strabismus); rapid, involuntary eye movements (nystagmus); unusual sensitivity to light (photophobia); clouding of the lenses of the eyes (cataracts); and/or a cone shape to the front of the eye (keratoconus). LCA is usually inherited as an autosomal recessive genetic condition. In addition, some infants may exhibit hearing loss, intellectual disability, and/or developmental delay.
Specific types of LCA have been defined based on the causative gene. Some types are associated with little change in vision over time (stationary disease) while others become more severe over time (progressive disease).
LCA is a monogenic disease and at least 27 genes are implicated. Changes (mutations) in these genes can account for about 80-90% of diagnosed cases of LCA. The genes responsible for the remaining 10-20% of diagnoses are not known. LCA is usually inherited as an autosomal recessive genetic condition. Twenty-four of the genes associated with LCA cause only recessive disease. Two genes (IMPDH1 and OTX2) are known to cause dominant disease. One gene (CRX) is known to cause either dominant or recessive disease, depending on the specific mutation.
Recessive genetic disorders occur when an individual inherits two copies of an abnormal gene for the same trait, one from each parent. If an individual receives one normal gene and one gene for the disease, the person will be a carrier for the disease but usually will not show symptoms. The risk for two carrier parents to both pass the defective gene and have an affected child is 25% with each pregnancy. The risk to have a child who is a carrier like the parents is 50% with each pregnancy. The chance for a child to receive normal genes from both parents and be genetically normal for that particular trait is 25%. The risk is the same for males and females.
There are about 20,000 different genes in a human and all individuals carry one copy of several abnormal genes. Parents who are close relatives (consanguineous) have a higher chance than unrelated parents to both carry the same abnormal gene, which increases the risk to have children with a recessive genetic disorder.
In rare cases, LCA is inherited as an autosomal dominant genetic disorder. Mutations in three genes, CRX, IMPDH1, and OTX2 are currently known to be associated with this type of LCA.
Dominant genetic disorders occur when only a single copy of an abnormal gene is necessary to cause a particular disease. The abnormal gene can be inherited from either parent or can be the result of a new mutation in the affected individual. The risk of passing the abnormal gene from affected parent to offspring is 50% for each pregnancy. The risk is the same for males and females.
Those affected populations with LCA:
The prevalence of LCA has been estimated to be 1-2/100,000 births. This disorder affects males and females in equal numbers.