“Liver failure is a life-threatening condition that demands urgent medical care. Most often, liver failure occurs gradually and over many years.”
WEB MD
“Liver failure is a life-threatening condition that demands urgent medical care. Most often, liver failure occurs gradually and over many years.”
WEB MD
“SIRS can be incited by ischemia, inflammation, trauma, infection or a combination of several “insults”. SIRS is not always associated with infection. While not universally accepted, some have proposed the terms “severe SIRS” and “SIRS shock” to describe serious clinical syndromes that are not infectious in nature and thus cannot be labeled according to the various sepsis definitions”
Steven D. Burdette M.D. (Infectious Disease Medicine M.D.– Wright State Physicians in Dayton, Ohio – http://www.healthgrades.com/physician/dr-steven-burdette-yhfgy)


Part 3 talks to you about the multi-hit theory of SIRS with Inflammatory Cascade of SIRS and lastly the coagulation process in SIRS. It also tells you an extensive amount of infectious and non-infectious causes of SIRS. Lastly the key antidote to SIRS.
Multi-hit theory
A multi hit theory behind the progression of SIRS to organ dysfunction and possibly multiple organ dysfunction syndrome (MODS). In this theory, the event that initiates the SIRS cascade primes the pump. With each additional event, an altered or exaggerated response occurs, leading to progressive illness. The key to preventing the multiple hits is adequate identification of the ETIOLOGY or CAUSE of SIRS and appropriate resuscitation and therapy.
Inflammatory cascade
Trauma, inflammation, or infection leads to the activation of the inflammatory cascade. Initially, a pro-inflammatory activation occurs, but almost immediately thereafter a reactive suppressing anti-inflammatory response occurs. This SIRS usually manifests itself as increased systemic expression of both pro-inflammatory and anti-inflammatory species. When SIRS is mediated by an infectious insult, the inflammatory cascade is often initiated by endotoxin or exotoxin. Tissue macrophages, monocytes, mast cells, platelets, and endothelial cells are able to produce a multitude of cytokines. The cytokines tissue necrosis factor–alpha (TNF-α) and interleukin-1 (IL-1) are released first and initiate several cascades.
The release of certain factors without getting into medical specific terms they ending line induces the production of other pro-inflammatory cytokines, worsening the condition.
Some of these factors are the primary pro-inflammatory mediators. In research it suggests that glucocorticoids may function by inhibit-ing certain factors that have been shown to be released in large quantities within 1 hour of an insult and have both local and systemic effects. In studies they have shown that certain cytokines given individually produce no significant hemodynamic response but that they cause severe lung injury and hypotension. Others responsible for fever and the release of stress hormones (norepinephrine, vasopressin, activation of the renin-angiotensin-aldosterone system).
Other cytokines, stimulate the release of acute-phase reactants such as C-reactive protein (CRP) and pro-calcitonin.
The pro-inflammatory interleukins either function directly on tissue or work via secondary mediators to activate the coagulation cascade and the complement cascade and the release of nitric oxide, platelet-activating factor, prostaglandins, and leukotrienes.
High mobility group box 1 (HMGB1) is a protein present in the cytoplasm and nuclei in a majority of cell types. In response to infection or injury, as is seen with SIRS, HMGB1 is secreted by innate immune cells and/or released passively by damaged cells. Thus, elevated serum and tissue levels of HMGB1 would result from many of the causes of SIRS.
HMGB1 acts as a potent pro-inflammatory cytokine and is involved in delayed endotoxin lethality and sepsis.
Numerous pro-inflammatory polypeptides are found within the complement cascade. It is thought they are felt to contribute directly to the release of additional cytokines and to cause vasodilatation and increasing vascular permeability. Prostaglandins and leukotrienes incite endothelial damage, leading to multi-organ failure.
Polymorphonuclear cells (PMNs) from critically ill patients with SIRS have been shown to be more resistant to activation than PMNs from healthy donors, but, when stimulated, demonstrate an exaggerated micro-bicidal response (agents that kill microbes). This may represent an auto-protective mechanism in which the PMNs in the already inflamed host may avoid excessive inflammation, thus reducing the risk of further host cell injury and death.[4]
Coagulation
The correlation between inflammation and coagulation is critical to understanding the potential progression of SIRS. IL-1 and TNF-α directly affect endothelial surfaces, leading to the expression of tissue factor. Tissue factor initiates the production of thrombin, thereby promoting coagulation, and is a proinflammatory mediator itself. Fibrinolysis is impaired by IL-1 and TNF-α via production of plasminogen activator inhibitor-1. Pro-inflammatory cytokines also disrupt the naturally occurring anti-inflammatory mediators anti-thrombin and activated protein-C (APC).
If unchecked, this coagulation cascade leads to complications of micro-vascular thrombosis, including organ dysfunction. The complement system also plays a role in the coagulation cascade. Infection-related pro-coagulant activity is generally more severe than that produced by trauma.
What the causes of SIRS can be:
The etiology of systemic inflammatory response syndrome (SIRS) is broad and includes infectious and noninfectious conditions, surgical procedures, trauma, medications, and therapies.
The following is partial list of the infectious causes of SIRS:
*PREVENTION IS THE KEY ANTIDOTE! So stay healthy and out of hospitals!*
“Systemic inflammatory response syndrome (SIRS), independent of the etiology, has the same pathophysiologic properties, with minor differences in inciting cascades.”
Dr. Lewis J. Kaplan (an MD of Yale Surgical Specialty Traumas, a medical author-http://emedicine.medscape.com/article/168943-overview#a0104)
It is the body’s response to an infectious or noninfectious insult. Although the definition of Systemic Inflammatory Response Syndrome (SIRS) refers to it as an “inflammatory” response, it actually has pro- and anti-inflammatory components. SIRS is a serious condition related to systemic inflammation, organ dysfunction, and organ failure. It is a subset of cytokine storm, in which there is abnormal regulation of various cytokines. Cytokines are this, the term “cytokine” is derived from a combination of two Greek words – “cyto” meaning cell and “kinos” meaning movement. Cytokines are cell messaging or signaling molecules that aid cell to cell communication in immune responses and stimulate the movement of cells towards sites of inflammation, infection and trauma.
Cytokines exist in peptide, protein and glycoprotein (proteins with a sugar attached) forms. The cytokines are a large family of molecules that are classified in various different ways due to an absence of a unified classification system. Protein is acidic as opposed to being alkalinic.
Examples of cytokines include the agents interleukin and the interferon which are involved in regulating the immune system’s response to inflammation and infection.
SIRS, independent of the etiology/cause, has the same pathophysiologic properties, with minor differences in inciting cascades. Many consider the syndrome a self-defense mechanism. Inflammation is the body’s response to nonspecific insults that arise from chemical, traumatic, or infectious stimuli. The inflammatory cascade is a complex process that involves humoral and cellular responses, complement, and cytokine cascades. Best summarized in the relationship between these complex interactions and SIRS is it is in the following 3-stage process. Here is a simple explanation in what occurs without taking pages in explaining the stages to you.
Stage I
Following an insult to the body, cytokines are produced at the site. Local cytokine production incites an inflammatory response, thereby promoting wound repair and recruitment of the reticular endothelial system. This process is essential for normal host defense homeostasis and if absent is not compatible with life. Local inflammation, such as in the skin and subcutaneous soft tissues occurs.
What occurs is rubor or redness at the site that reflects local vasodilation of vessels. What is caused by release of local vasodilation of the vessels at the area of where the insult starts in the body is substances like nitric oxide (NO) and prostacyclin get released=Acidic.
Tumor or swelling occurs due to vascular endothelial (layer of the skin) tight junction disruption and the local extravasation of protein-rich fluid into the interstitium (layer of the skin), which also allows activated white blood cells to pass from the vascular space (blood stream) into the tissue space to help clear infection and promote repair.
Dolor is pain and represents the impact inflammatory mediators have on local somatosensory nerves. Presumably, this pain stops the host from trying to use this part of his or her body as it tries to repair itself.
The increased heat primarily due to increased blood flow occurs but also increased local metabolism as white blood cells become activated and localize to the injured tissue.
Finally, the loss of function, a hallmark of inflammation and a common clinical finding of organ dysfunction with the infection is isolated to a specific organ (ex. pneumonia—acute respiratory failure; kidney—acute kidney injury. pancreatitis– inflammation of the pancreas).
Importantly, on a local level, this cytokine and chemokine release by attracting activated leukocytes to the region may cause local tissue destruction (ex. abscess) or cellular injury (ex. pus), which appear to be the necessary byproducts of an effective local inflammatory response. Local infection signs & symptoms= puss, swelling. skin temperature hot, pain and redness to the where the insult of the body is.
Ending line what happens is an insult occurs in the body, there is local cytokine production with the goal of inciting an inflammatory response thereby promoting wound repair and recruitment of the reticular endothelial system. Your body is compensating in reacting normally to this insult.
Stage II
Small quantities of local cytokines are released into the circulation, improving the local response. This leads to growth factor stimulation and the recruitment of macrophages and platelets. This acute phase response is typically well controlled by a decrease in the pro-inflammatory mediators and by the release of endogenous antagonists; the goal is homeostasis. At this stage, some minimal malaise (general weakness)and low-grade fever may become show.
Putting it simple what occurs here is small quantities of local cytokines are released into circulation to improve the local response. This leads to growth factor stimulation and the recruitment of macrophages (cells eating up toxins to the body) and platelets (that are cells the coagulate-cause clotting). This acute phase response is typically well controlled by a decrease in the proinflammatory mediators and by the release of endogenous antagonists. The goal is homeostasis – the body still trying to compensate and react productively to this insult to the body.
Stage III
If homeostasis is not restored and if the inflammatory stimuli continue to seed into the systemic circulation, a significant systemic reaction occurs. The cytokine release (acidic) leads to destruction rather than protection. A consequence of this is the activation of numerous humoral cascades and the activation of the reticular endothelial system and subsequent loss of circulatory integrity. The body at this stage is decompensating and not productively fighting off this insult to the body and this leads to end-organ dysfunction.
Tune in tomorrow to part 3 of SIRS the conclusion of this topic (extensive noninfectious and infectious causes with more on coagulation and multi cascading reactions in the body due to SIRS).
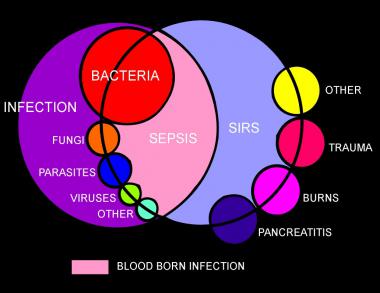
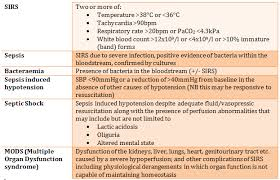
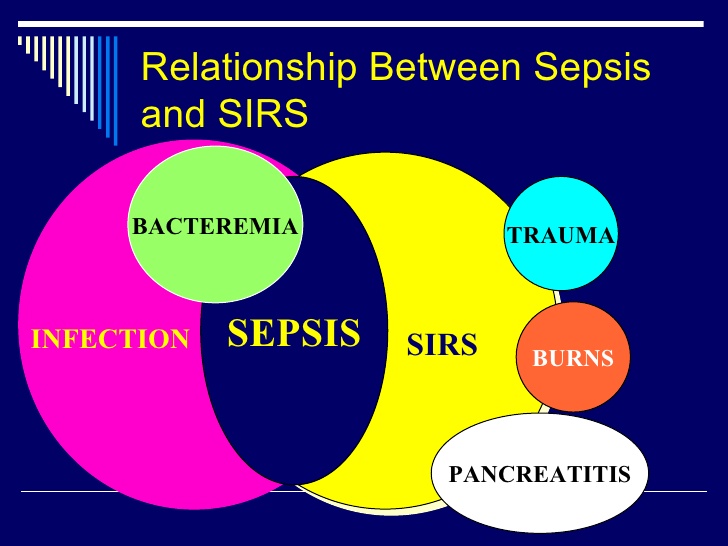
What is SIRS? SIRS was first described by Dr William R. Nelson, of the University of Toronto, in a presentation to the Nordic Micro Circulation meeting in Geilo, Norway-February 1983. In 1992, the American College of Chest Physicians (ACCP) and the Society of Critical Care Medicine (SCCM) introduced definitions for systemic inflammatory response syndrome (SIRS), sepsis, severe sepsis, septic shock, and multiple organ dysfunction syndrome (MODS), they are interrelated with each other in SIRS. The idea behind defining SIRS was to define a clinical response to a nonspecific insult of either infectious or noninfectious origin. SIRS is defined as 2 or more of the following variables:
The doctor also administers IV fluids to prevent blood pressure from dropping too low. In some cases, vasopressor medications (which constrict blood vessels) are needed to achieve an adequate blood pressure. Some patients are given new drug therapies, such as activated protein C (APC). And finally, if organ failures occur, appropriate supportive care is provided (for example, dialysis for kidney failure, mechanical ventilation for respiratory failure, etc.). Commonly what is used when initially sepsis is diagnosed is Vancomycin with other antibiotics like Imipenum, Cefepime, and others depending on what the blood culture shows as the microorganism if SIRS is caused by a bacterial infection (many times it is).
QUOTE FOR THURSDAY:
“Current theories about the onset and progression of sepsis and SIRS focus on dysregulation of the inflammatory response, including the possibility that a massive and uncontrolled release of proinflammatory mediators initiates a chain of events that lead to widespread tissue injury.”
Dr. Remi Neviere, MD/Professor/Author of Sepsis and the systemic inflammatory response syndrome: MD Department of Physiology, Univ. Droit et Sante – Lille II
Go to striveforgoodhealth.com and learn about a vital occurrence happening in hospitals for years called SIRS=Systemic Inflammatory Response Syndrome.
Virginia Postrel (born January 14, 1960 is an American political and a cultural writer).
“Excess dietary salt is most notorious for increasing blood pressure. Americans have a 90 percent lifetime probability of developing high blood pressure – so even if your blood pressure is normal now, if you continue to eat the typical American diet, you will be at risk.“
Joel Fuhrman M.D. (born December 2, 1953), is an American board-certified family physician who specializes in nutrition-based treatments for obesity and chronic disease.

The foods to buy are low sodium foods —-What to buy:
–Fruits – Fresh, canned or frozen. I recommend with canned look at the ingredients to make sure you know how much sodium is in a serving. Remember for a person with high b/p you want to keep your sodium count less than 1800 to 2000mg a day. Sodium causes the vessels to vasoconstrict (or narrow) which increases blood pressure in a person.
-Vegetables – Fresh or frozen (no sauce or plastic pouches) Canned (UNSALTED, AGAIN check the canned label for the amount of sodium in each serving.).
–Drinks – Fruits juices, fresh or frozen.
Canned low sodium or no salt added tomato & vegetable juice.
Instant breakfast* (all flavors but eggnog) —- limit to 1 cup /day
-Dairy choices – liguid or dry milk (1% or skim milk).
Homemade buttermilk (made from powdered milk) *limit these to 2-3 cups a day*
Cottage cheese, dry cured (low sodium)
Ricotta Cheese from low fat or skim milk
Farmer Cheese, part skim mozzarella neufchated *limit cheese to 1oz or 1/2 cup of one cheese/day.
-Fats, Oils – Canola, Olive, Corn, Cottonseed, Peanut, Safflower, Soybean &
Margarine (unsalted)
–Meats, Poultry, Fish
Fish, fresh or frozen (NOT BREADED): Canned tuna and salmon (Unsalted or rinsed).
Chicken or Turkey
Lean cuts of: BEEF, VEAL, PORK, LAMB.
BEEF TONGUE if you must have.
-Meat Substitutes
Dried beans, peas, lentils (not canned)
Nuts or seeds (UNSALTED, DRY ROASTED), sunflower seeds, peanuts, almonds, walnuts.
Unsalted peanut butter
Tofu (soybean curd)
–Breads, Cerals, Grains, Starches:
Loaf of bread and yeast rolls (limit to 3 slices a day)
Homemade breads with regular flour, not self rising.
Melba Toast
Matzo Crackers
Pita Bread
Taco Shell
Tortilla (corn)
Cooked cereals like corn grits, farina (regular), oatmeal, oat bran, cream of rice, cream of wheat (AVOID instant cereals).
Puffed Rice or wheat, shredded wheat (or any cereal with 100-150mg sodium–limit to 1 cup a day).
Wheat germ
Popcorn (no salt or fat added)
Starchy vegetables: corn, potato, green beans, etc… (not canned unless salt free).
Rice (enriched white or brown)
Pasta
– Cooking ingredients, seasonings
Corn starch, tapioca
Corn meal (not self rising)
Fresh or dried herbs, salt free herb seasonings.
Flour, regular white or whole wheat (not self rising)
Fresh fruits or vegetables (lemons, limes, onions, celery, etc.)
Fresh garlic or ginger
Louisiana – type hot sauce (limit to 1 tsp/day)
Low sodium baking powder
Onion or garlic powder
Tomato paste, unsalted tomatoes, unsalted tomato sauce.
Vinegar
Water chestnuts, yeast, butter substitute (such as Molly Mc Butter—limit to 1/2 tsp/day).
– Sweets
Carob powder, cocoa powder
Flavored gelatins
Fruits (fresh, canned, frozen)
Frozen juice bars, fruit ice, sorbet, sherbet
Sugar, honey, molasses, syrup (cane or maple)
Jelly, jams, preserves, apple butter
Graham and animal crackers, fig bars, ginger snaps
OTHER WAYS TO IMPROVE HEART FUNCTION:
**Recommended is to get clearance for any changes you decide to make with this advice on blood pressure since you may have other conditions that may not allow certain food, or activity changes. If you have high blood pressure get yourself a cardiologist if you don’t have one yet and is a specialist in knowing the best treatment for you.**