“Sometimes, it’s just easier to say yes to that extra snack or dessert, because frankly, it is exhausting to keep saying no. It’s exhausting to plead with our kids to eat just one more bite of vegetables.”
Michelle Obama
“Sometimes, it’s just easier to say yes to that extra snack or dessert, because frankly, it is exhausting to keep saying no. It’s exhausting to plead with our kids to eat just one more bite of vegetables.”
Michelle Obama
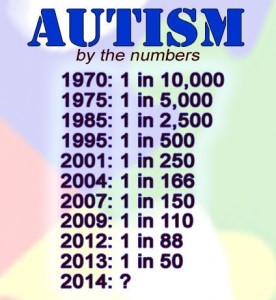
“Today, the Centers for Disease Control and Prevention (CDC) announced that the incidence rate of autism among eight year olds in the United States remains 1 out of 68 children. This updated report occurs every two years, with the previous report being released from the CDC in April 2014.”
Autism Society . Org
Autism spectrum disorder (ASD) refers to a group of complex neurodevelopment disorders characterized by repetitive and characteristic patterns of behavior and difficulties with social communication and interaction. The symptoms are present from early childhood and affect daily functioning.
The term “spectrum” refers to the wide range of symptoms, skills, and levels of disability in functioning that can occur in people with ASD. Some children and adults with ASD are fully able to perform all activities of daily living while others require substantial support to perform basic activities. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5, published in 2013) includes Asperger syndrome, childhood disintegrative disorder, and pervasive developmental disorders not otherwise specified (PDD-NOS) as part of ASD rather than as separate disorders. A diagnosis of ASD includes an assessment of intellectual disability and language impairment.
ASD occurs in every racial and ethnic group, and across all socioeconomic levels. However, boys are significantly more likely to develop ASD than girls. The latest analysis from the Centers for Disease Control and Prevention estimates that 1 in 68 children has ASD.
What are some common signs of ASD?
Even as infants, children with ASD may seem different, especially when compared to other children their own age. They may become overly focused on certain objects, rarely make eye contact, and fail to engage in typical babbling with their parents. In other cases, children may develop normally until the second or even third year of life, but then start to withdraw and become indifferent to social engagement.
The severity of ASD can vary greatly and is based on the degree to which social communication, insistence of sameness of activities and surroundings, and repetitive patterns of behavior affect the daily functioning of the individual.
Social impairment and communication difficulties Many people with ASD find social interactions difficult. The mutual give-and-take nature of typical communication and interaction is often particularly challenging. Children with ASD may fail to respond to their names, avoid eye contact with other people, and only interact with others to achieve specific goals. Often children with ASD do not understand how to play or engage with other children and may prefer to be alone. People with ASD may find it difficult to understand other people’s feelings or talk about their own feelings.
People with ASD may have very different verbal abilities ranging from no speech at all to speech that is fluent, but awkward and inappropriate. Some children with ASD may have delayed speech and language skills, may repeat phrases, and give unrelated answers to questions. In addition, people with ASD can have a hard time using and understanding non-verbal cues such as gestures, body language, or tone of voice. For example, young children with ASD might not understand what it means to wave goodbye. People with ASD may also speak in flat, robot-like or a sing-song voice about a narrow range of favorite topics, with little regard for the interests of the person to whom they are speaking.
Repetitive and characteristic behaviors Many children with ASD engage in repetitive movements or unusual behaviors such as flapping their arms, rocking from side to side, or twirling. They may become preoccupied with parts of objects like the wheels on a toy truck. Children may also become obsessively interested in a particular topic such as airplanes or memorizing train schedules. Many people with ASD seem to thrive so much on routine that changes to the daily patterns of life — like an unexpected stop on the way home from school — can be very challenging. Some children may even get angry or have emotional outbursts, especially when placed in a new or overly stimulating environment.
What disorders are related to ASD?
Certain known genetic disorders are associated with an increased risk for autism, including Fragile X syndrome (which causes intellectual disability) and tuberous sclerosis (which causes benign tumors to grow in the brain and other vital organs) — each of which results from a mutation in a single, but different, gene. Recently, researchers have discovered other genetic mutations in children diagnosed with autism, including some that have not yet been designated as named syndromes. While each of these disorders is rare, in aggregate, they may account for 20 percent or more of all autism cases.
People with ASD also have a higher than average risk of having epilepsy. Children whose language skills regress early in life — before age 3 — appear to have a risk of developing epilepsy or seizure-like brain activity. About 20 to 30 percent of children with ASD develop epilepsy by the time they reach adulthood. Additionally, people with both ASD and intellectual disability have the greatest risk of developing seizure disorder.
How is ASD diagnosed?
ASD symptoms can vary greatly from person to person depending on the severity of the disorder. Symptoms may even go unrecognized for young children who have mild ASD or less debilitating handicaps. Very early indicators that require evaluation by an expert include:
Later indicators include:
Health care providers will often use a questionnaire or other screening instrument to gather information about a child’s development and behavior. Some screening instruments rely solely on parent observations, while others rely on a combination of parent and doctor observations. If screening instruments indicate the possibility of ASD, a more comprehensive evaluation is usually indicated.
A comprehensive evaluation requires a multidisciplinary team, including a psychologist, neurologist, psychiatrist, speech therapist, and other professionals who diagnose and treat children with ASD. The team members will conduct a thorough neurological assessment and in-depth cognitive and language testing. Because hearing problems can cause behaviors that could be mistaken for ASD, children with delayed speech development should also have their hearing tested.
What causes ASD?
Scientists believe that both genetics and environment likely play a role in ASD. There is great concern that rates of autism have been increasing in recent decades without full explanation as to why. Researchers have identified a number of genes associated with the disorder. Imaging studies of people with ASD have found differences in the development of several regions of the brain. Studies suggest that ASD could be a result of disruptions in normal brain growth very early in development. These disruptions may be the result of defects in genes that control brain development and regulate how brain cells communicate with each other. Autism is more common in children born prematurely. Environmental factors may also play a role in gene function and development, but no specific environmental causes have yet been identified. The theory that parental practices are responsible for ASD has long been disproved. Multiple studies have shown that vaccination to prevent childhood infectious diseases does not increase the risk of autism in the population.
What role do genes play?
Twin and family studies strongly suggest that some people have a genetic predisposition to autism. Identical twin studies show that if one twin is affected, then the other will be affected between 36 to 95 percent of the time. There are a number of studies in progress to determine the specific genetic factors associated with the development of ASD. In families with one child with ASD, the risk of having a second child with the disorder also increases. Many of the genes found to be associated with autism are involved in the function of the chemical connections between brain neurons (synapses). Researchers are looking for clues about which genes contribute to increased susceptibility. In some cases, parents and other relatives of a child with ASD show mild impairments in social communication skills or engage in repetitive behaviors. Evidence also suggests that emotional disorders such as bipolar disorder and schizophrenia occur more frequently than average in the families of people with ASD.
In addition to genetic variations that are inherited and are present in nearly all of a person’s cells, recent research has also shown that de novo, or spontaneous, gene mutations can influence the risk of developing autism spectrum disorder. De novo mutations are changes in sequences of deoxyribonucleic acid or DNA, the hereditary material in humans, which can occur spontaneously in a parent’s sperm or egg cell or during fertilization. The mutation then occurs in each cell as the fertilized egg divides. These mutations may affect single genes or they may be changes called copy number variations, in which stretches of DNA containing multiple genes are deleted or duplicated. Recent studies have shown that people with ASD tend to have more copy number de novo gene mutations than those without the disorder, suggesting that for some the risk of developing ASD is not the result of mutations in individual genes but rather spontaneous coding mutations across many genes. De novo mutations may explain genetic disorders in which an affected child has the mutation in each cell but the parents do not and there is no family pattern to the disorder. Autism risk also increases in children born to older parents. There is still much research to be done to determine the potential role of environmental factors on spontaneous mutations and how that influences ASD risk.
Do symptoms of autism change over time?
For many children, symptoms improve with age and behavioral treatment. During adolescence, some children with ASD may become depressed or experience behavioral problems, and their treatment may need some modification as they transition to adulthood. People with ASD usually continue to need services and supports as they get older, but depending on severity of the disorder, people with ASD may be able to work successfully and live independently or within a supportive environment.
How is autism treated?
There is no cure for ASD. Therapies and behavioral interventions are designed to remedy specific symptoms and can substantially improve those symptoms. The ideal treatment plan coordinates therapies and interventions that meet the specific needs of the individual. Most health care professionals agree that the earlier the intervention, the better.
Educational/behavioral interventions: Early behavioral/educational interventions have been very successful in many children with ASD. In these interventions therapists use highly structured and intensive skill-oriented training sessions to help children develop social and language skills, such as applied behavioral analysis, which encourages positive behaviors and discourages negative ones. In addition, family counseling for the parents and siblings of children with ASD often helps families cope with the particular challenges of living with a child with ASD.
Medications: While medication can’t cure ASD or even treat its main symptoms, there are some that can help with related symptoms such as anxiety, depression, and obsessive-compulsive disorder. Antipsychotic medications are used to treat severe behavioral problems. Seizures can be treated with one or more anticonvulsant drugs. Medication used to treat people with attention deficit disorder can be used effectively to help decrease impulsivity and hyperactivity in people with ASD. Parents, caregivers, and people with autism should use caution before adopting any unproven treatments
“After a century of studying schizophrenia, the cause of the disorder remains unknown.”
Thomas R. Insel (born October 19, 1951) is an American neuroscientist and psychiatrist who led the National Institute of Mental Health (NIMH) from 2002 until November 2015
Schizophrenia is a serious disorder which effects how a person thinks, feels and acts. A individual with this diagnosis may have difficulty distinguishing between what is real and what is imaginary; may be unresponsive or withdrawn; and may have difficulty expressing normal emotions in social situations. The person with schizophrenia may have difficulty expressing normal emotions in social situations.
Contrary to public perception, schizophrenia is not split personality or multiple ones. The vast majority of people with schizophrenia are not violent and do not pose a danger to others; if anyone they could put a danger to is themselves without supervision around. Schizophrenia is not caused by childhood experiences, poor parenting, lack of will power. The signs and symptoms of the disease are not the same for each person.
The cause of schizophrenia is still not clear.
Some theories about the cause of this disease include: genetics (heredity), biology (the imbalance in the brain’s chemistry); and/or possible viral infections and immune disorders.
One possible cause can be genetics (heredity). Scientists recognize that the disorder tends to run in families and a person inherits to develop the disease. Schizophrenia may also be triggered by environmental events like viral infections or highly stressful situations or a combination of both. Similar to some other genetically-related illnesses, schizophrenia appears when the body undergoes hormonal and physical changes, like those that occur during puberty in the teen and young adult years.
Another possible cause is Substance Use. Some studies have suggested that taking mind-altering drugs during teen years and young adulthood can increase the risk of schizophrenia. A growing body of evidence indicates that smoking marijuana increases the risk of psychotic incidents and the risk of ongoing psychotic experiences. The younger and more frequent the use, the greater the risk. Another study has found that smoking marijuana led to earlier onset of schizophrenia and often preceded the manifestation of the illness.
Another high possible cause deals with chemistry. Genetics help to determine huw the brain uses certain chemicals. People with schitzophrenia have a chemical imbalance of brain chemicals (serotonin and dopamine) which are neurotransmitters. These neurotransmitters allow nerve cells in the brain that send messages to each nerve cell. The brain is made up of nerve cells, called neurons, and chemicals, called neurotransmitters. An imbalance of one neurotransmitter, dopamine, is thought to cause the symptoms of schizophrenia. … The “dopamine hypothesis” has been the main theory regarding the cause of the symptoms of schizophrenia. Dopamine is produced in the dopaminergic neurons in the ventral tegmental area (VTA) of the midbrain, the substantia nigra pars compacta, and the arcuate nucleus of the hypothalamus. With the imbalance these chemicals affects the way a person’s brain reacts to stimuli—which explains why a person with schizophrenia may be overwhelmed by sensory information (Ex. loud music or bright lights) which other people can easily handle. This problem in processing different sounds, sights, smells and tastes can also lead to hallucinations or delusions.
Looking for a moment at Dopamine in different areas of the brain in both low and high amounts see how it effects brain thinking to better understand schizophrenia.
Dopamine in cognition:
Dopamine in the frontal lobes of the brain controls the flow of information from other areas of the brain. Disorders of dopamine in this region lead to decline in neurocognitive functions, especially memory, attention, and problem-solving.
D1 receptors and D4 receptors are responsible for the cognitive-enhancing effects of dopamine. Some of the antipsychotic medications used in conditions like schizophrenia act as dopamine antagonists. Older, so-called “typical” antipsychotics most commonly act on D2 receptors, while the atypical drugs also act on D1, D3 and D4 receptors.
Dopamine in movement
A part of the brain called the basal ganglia regulates movement. Basal ganglia in turn depend on a certain amount of dopamine to function at peak efficiency. The action of dopamine occurs via dopamine receptors, D1-5.
Dopamine reduces the influence of the indirect pathway, and increases the actions of the direct pathway within the basal ganglia. When there is a deficiency in dopamine in the brain, movements may become delayed and uncoordinated. On the flip side, if there is an excess of dopamine, the brain causes the body to make unnecessary movements, such as repetitive tics.
Dopamine in pleasure reward seeking behavior
Dopamine is the chemical that mediates pleasure in the brain. It is released during pleasurable situations and stimulates one to seek out the pleasurable activity or occupation. This means food, sex, and several drugs of abuse are also stimulants of dopamine release in the brain, particularly in areas such as the nucleus accumbens and prefrontal cortex.
Dopamine and addiction
Cocaine and amphetamines inhibit the re-uptake of dopamine. Cocaine is a dopamine transporter blocker that competitively inhibits dopamine uptake to increase the presence of dopamine.
Amphetamine increases the concentration of dopamine in the synaptic gap, but by a different mechanism. Amphetamines are similar in structure to dopamine, and so can enter the presynaptic neuron via its dopamine transporters. By entering, amphetamines force dopamine molecules out of their storage vesicles. By increasing presence of dopamine both these lead to increased pleasurable feelings and addiction.
Dopamine in memory
Levels of dopamine in the brain, especially the prefrontal cortex, help in improved working memory. However, this is a delicate balance and as levels increase or decrease to abnormal levels, memory suffers.
Dopamine in attention
Dopamine helps in focus and attention. Vision helps a dopamine response in the brain and this in turn helps one to focus and direct their attention. Dopamine may be responsible for determining what stays in the short term memory based on an imagined response to certain information. Reduced dopamine concentrations in the prefrontal cortex are thought to contribute to attention deficit disorder.
Dopamine is affected in schizophrenia, just look at the functions of the chemical and the signs and symptoms of schizophrenia.
Signs and symptoms of schizophrenia:
–Deficits in cognitive abilities are widely recognized as a core feature of this disease. The deficits impacting the cognitive function are found in a large number of areas: working memory, long-term memory,verbaldeclarative memory, semantic processing, episodic memory, attention, learning (particularly verbal learning). Deficits in verbal memory are the most pronounced in individuals with schizophrenia, and are not accounted for by deficit in attention. Verbal memory impairment has been linked to a decreased ability in individuals with schizophrenia to semantically encode (process information relating to meaning), which is cited as a cause for another known deficit in long-term memory. When given a list of words, healthy individuals remember positive words more frequently (known as the Pollyanna principle); however, individuals with schizophrenia tend to remember all words equally regardless of their connotations, suggesting that the experience of anhedonia impairs the semantic encoding of the words. These deficits have been found in individuals before the onset of the illness to some some extent and varying degrees.
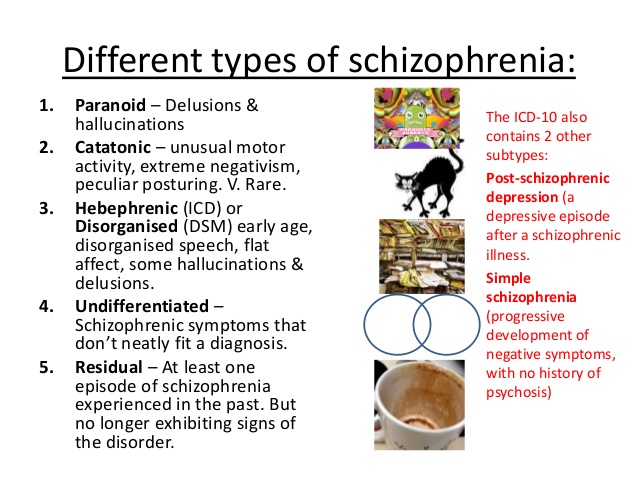
-Delusions
-Hallucinations
-Disorganized speech
-Disorganized or catatonic behavior
TREATMENT FOR SCHIZOPHRENIA:
There is no cure for schizophrenia, but it can be treated and managed in several ways.
-Antipsychotic medications
-Psychotherapy, such as cognitive behavioral therapy and assertive community treatment and supportive therapy.
– Self-management strategies and education
“Highly concentrated sources of oxygen promote rapid combustion and therefore are fire and explosion hazards in the presence of fuels. The fire that killed the Apollo 1 crew on a test launchpad spread so rapidly because the pure oxygen atmosphere was at normal atmospheric pressure instead of the one third pressure that would be used during an actual launch.”
LENNTECH.com http://www.lenntech.com/periodic/elements/o.htm#ixzz48HfY7per Water Treatment and Purification Company
“Oxygen, although it is essential for aerobic organisms for respiration as well as energy production, has been therapeutically used for a long time. It also can be either toxic or lethal for humans if it is continuously inhaled pure for about 60 hours.”
U.S. National Library of Medicine/National Institute of Health http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3231820/
“When you exhaust all possibilities remember this: You haven’t!”
Thomas Edison (Inventor and Businessman)
“When you exhaust all possibilities remember this: You haven’t!”
Thomas Edison (Inventor and Businessman)
By definition, Parkinson’s is a progressive disease. Although some people with Parkinson’s only have symptoms on one side of the body for many years, eventually the symptoms begin on the other side.
Parkinson’s Disease Foundation