“It is easier to find men who will volunteer to die, than to find those who are willing to endure pain with patience.”
Julius Caesar
“It is easier to find men who will volunteer to die, than to find those who are willing to endure pain with patience.”
Julius Caesar
‘This is potentially a very important discovery which may go a long way to explain the marked differences in pain sensitivity and chronicity between women and men.”
says James McRoberts, a pain researcher at the University of California-Los Angeles
“When a loved one dies, you might be faced with grief over your loss again and again — sometimes even years later. Feelings of grief might return on the anniversary of your loved one’s death, birthday or other special days throughout the year. This is called anniversary reaction, its not a set back. You’re reflecting memories and that this loved one was important to you. To continue on the path toward healing, know what to expect — and how to cope with reminders of your loss.”
MAYO CLINIC
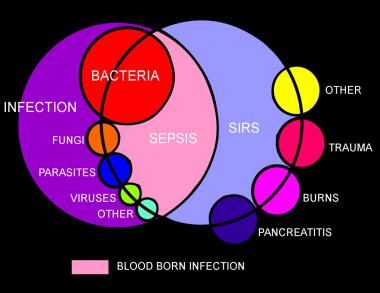
“Sepsis is the systemic response to infection and is defined as the presence of SIRS (systemic inflammatory response syndrome) in addition to a documented or presumed infection.”
Part 3 talks to you about the multi-hit theory of SIRS with Inflammatory Cascade of SIRS and lastly the coagulation process in SIRS. It also tells you an extensive amount of infectious and non-infectious causes of SIRS. Lastly the key antidote to SIRS.
Multi-hit theory
A multi hit theory behind the progression of SIRS to organ dysfunction and possibly multiple organ dysfunction syndrome (MODS). In this theory, the event that initiates the SIRS cascade primes the pump. With each additional event, an altered or exaggerated response occurs, leading to progressive illness. The key to preventing the multiple hits is adequate identification of the ETIOLOGY or CAUSE of SIRS and appropriate resuscitation and therapy.
Inflammatory cascade
Trauma, inflammation, or infection leads to the activation of the inflammatory cascade. Initially, a pro-inflammatory activation occurs, but almost immediately thereafter a reactive suppressing anti-inflammatory response occurs. This SIRS usually manifests itself as increased systemic expression of both pro-inflammatory and anti-inflammatory species. When SIRS is mediated by an infectious insult, the inflammatory cascade is often initiated by endotoxin or exotoxin. Tissue macrophages, monocytes, mast cells, platelets, and endothelial cells are able to produce a multitude of cytokines. The cytokines tissue necrosis factor–alpha (TNF-α) and interleukin-1 (IL-1) are released first and initiate several cascades.
The release of certain factors without getting into medical specific terms they ending line induces the production of other pro-inflammatory cytokines, worsening the condition.
Some of these factors are the primary pro-inflammatory mediators. In research it suggests that glucocorticoids may function by inhibit-ing certain factors that have been shown to be released in large quantities within 1 hour of an insult and have both local and systemic effects. In studies they have shown that certain cytokines given individually produce no significant hemodynamic response but that they cause severe lung injury and hypotension. Others responsible for fever and the release of stress hormones (norepinephrine, vasopressin, activation of the renin-angiotensin-aldosterone system).
Other cytokines, stimulate the release of acute-phase reactants such as C-reactive protein (CRP) and pro-calcitonin.
The pro-inflammatory interleukins either function directly on tissue or work via secondary mediators to activate the coagulation cascade and the complement cascade and the release of nitric oxide, platelet-activating factor, prostaglandins, and leukotrienes.
High mobility group box 1 (HMGB1) is a protein present in the cytoplasm and nuclei in a majority of cell types. In response to infection or injury, as is seen with SIRS, HMGB1 is secreted by innate immune cells and/or released passively by damaged cells. Thus, elevated serum and tissue levels of HMGB1 would result from many of the causes of SIRS.
HMGB1 acts as a potent pro-inflammatory cytokine and is involved in delayed endotoxin lethality and sepsis.
Numerous pro-inflammatory polypeptides are found within the complement cascade. It is thought they are felt to contribute directly to the release of additional cytokines and to cause vasodilatation and increasing vascular permeability. Prostaglandins and leukotrienes incite endothelial damage, leading to multi-organ failure.
Polymorphonuclear cells (PMNs) from critically ill patients with SIRS have been shown to be more resistant to activation than PMNs from healthy donors, but, when stimulated, demonstrate an exaggerated micro-bicidal response (agents that kill microbes). This may represent an auto-protective mechanism in which the PMNs in the already inflamed host may avoid excessive inflammation, thus reducing the risk of further host cell injury and death.[4]
Coagulation
The correlation between inflammation and coagulation is critical to understanding the potential progression of SIRS. IL-1 and TNF-α directly affect endothelial surfaces, leading to the expression of tissue factor. Tissue factor initiates the production of thrombin, thereby promoting coagulation, and is a proinflammatory mediator itself. Fibrinolysis is impaired by IL-1 and TNF-α via production of plasminogen activator inhibitor-1. Pro-inflammatory cytokines also disrupt the naturally occurring anti-inflammatory mediators anti-thrombin and activated protein-C (APC).
If unchecked, this coagulation cascade leads to complications of micro-vascular thrombosis, including organ dysfunction. The complement system also plays a role in the coagulation cascade. Infection-related pro-coagulant activity is generally more severe than that produced by trauma.
What the causes of SIRS can be:
The etiology of systemic inflammatory response syndrome (SIRS) is broad and includes infectious and noninfectious conditions, surgical procedures, trauma, medications, and therapies.
The following is partial list of the infectious causes of SIRS:
“SIRS can be incited by ischemia, inflammation, trauma, infection or a combination of several “insults”. SIRS is not always associated with infection. While not universally accepted, some have proposed the terms “severe SIRS” and “SIRS shock” to describe serious clinical syndromes that are not infectious in nature and thus cannot be labeled according to the various sepsis definitions”
Steven D. Burdette M.D. (Infectious Disease Medicine M.D.– Wright State Physicians in Dayton, Ohio – http://www.healthgrades.com/physician/dr-steven-burdette-yhfgy)
“The idea behind defining SIRS was to define a clinical response to a nonspecific insult of either infectious or noninfectious origin. In 1992, the American College of Chest Physicians (ACCP) and the Society of Critical Care Medicine (SCCM) introduced definitions for systemic inflammatory response syndrome (SIRS), sepsis, severe sepsis, septic shock, and multiple organ dysfunction syndrome MODS).”
“Current theories about the onset and progression of sepsis and SIRS focus on dysregulation of the inflammatory response, including the possibility that a massive and uncontrolled release of proinflammatory mediators initiates a chain of events that lead to widespread tissue injury.”
Dr. Remi Neviere, MD/Professor/Author of Sepsis and the systemic inflammatory response syndrome: Definitions, epidemiology, and prognosis http://www.uptodate.com/contents/sepsis-and-the-systemic-inflammatory-response-syndrome-definitions-epidemiology-and-prognosis & http://circ.ahajournals.org/content/111/20/2596
MD Department of Physiology, Univ. Droit et Sante – Lille II
Albert Einstein (14 March 1879 – 18 April 1955) was a German-born theoretical physicist

Cellulite in technical terms is noted at adiposis edematoso meaning your adipose tissue=fat that has swollen up (edematoso); or it is called gynoid lipodystrophy meaning anything pertaining to the women (gynoid) and that the lipid tissue is degenerating (ending line loosing tone). One other medical term it is noted as is orange peel syndrome=the herniation of subcutaneous fat within fibrous connective tissue that ends up looking like skin dimpling, often on the pelvic region (Specifically the buttock) including the lower limbs (thighs) and abdomen. Cellulite occurs in most postpubescent females and rarely in males. Why is this? Well, for one the tissue make up some say that men’s tissue in these areas are made up in a horizontal make up where in women it’s a honey comb make up allowing more fat to store. That is why you see most men overweight with it in the abdomen and not in the legs or buttock compared to women. Also with women in menopause the hormonal make up compared to men which adds to increasing the chance of putting weight on. The factors that can prone you to cellulite forming on the body are 1-genetic (which may be the biggest factor in developing it especially if it’s in the family tree), 2-hormones (Estrogen the important hormone to initiate and aggravate cellulite.), 3-predisposing factors (Sex, race, biotype, or predisposition to lymphatic or circulatory insufficiency which contribute to cellulite), 4-Let’s not forget lifestyle also (increase in level of catecholamines, which associate with the evolution of cellulite (particularly sedentary lifestyle). Lack of activity (not work out) but walking fast 30 to 60 minutes a day would surely show a difference in your cellulite in time with good healthy dieting.
Problems that cause cellulite to show on your body is poor health habits, poor dieting to the point you get overweight or obese. Eat meals low in starches & carbohydrates, low in sugar, and moderate amounts of fat. With your protein highest in count of every meal (about 14 or so in 6 meals a day is more than enough) and by the end of the day your protein count should add up to the highest number compared to the others. Why because you keep your metabolism at a steady rate with your sugar count not spiking into high levels of glucose in your bloodstream, after a meal. What is so important about this? Realize that starches, carbohydrates (CHOs), sugars=calories and some fats will get broken down into complex or simple sugars (frucose and glucose for example) during the digestion process in the stomach. Eating only 3 to 4 large or moderate or even small meals high in sugar, CHOs, starches or fat=ending product of high spikes of sugar in your blood stream. In doing this your body naturally reacts, first sending glucose in the bloodstream to the pancreas. The pancreas senses glucose in the blood then releases the hormone insulin (not like in diabetics since their pancreas will release nonworking insulin or too little of working insulin to no insulin at all). The insulin will allow the glucose to transfer into tissues and cells that are utilizing the need for sugar which is our fuel/energy but only for the amount needed at that time. Usually glucose is our primary fuel to tissues and cells to allow them to do their function-like gas to a car to be able to run; but remember our human body can’t release the extra glucose out of our body left in the blood stream that came from our breakdown, in our stomach, from our meal. When the glucose was needed in the body cells and tissues, at that time, it was used but not all was utilized we don’t utilize all that sugar especially if it is a large meal or even a moderate to small meal that had high sugar or carbohydrates or starch in it. These kind of meals produce excess sugar in the blood stream. Now if the body could just release extra sugar from the body as a waste product (through urine or stool or perspiration) no one would be overweight or obese in any country and we could eat anything we want (from eggs benedict every day for breakfast to burger king hamburger with fries on it for lunch to Chinese fast food with Sundaes for dinner and of course let’s not forget milk chocolate for snacks in between). The body doesn’t work that way. The excess sugar your body didn’t need to utilize at that time now goes to the liver where this organ converts glucose to glycogen (from active sugar to inactive sugar). So when needed (glucose), the liver can just release glycogen into the blood stream where it gets converted back to glucose if the body needs active energy at that time (If you’re doing a 16 hr shift with you now into 12hrs of your shift and no food since 6am the body needs fuel at that point the liver will do this releasing of glycogen to the bloodstream, for example); but if you’re eating 3 large or moderate meals a day with snacks in between the liver won’t need to do this releasing of glycogen into the bloodstream, especially if you’re not eating healthy but fast foods or not working out 3 to 5 times a week with working 40 hours a week or equating to be that active in your life. Now remember your liver is only so big to store a certain amount of glucose and when it reaches full the sugar that couldn’t get stored in the liver than stays in the blood stream. The glucose has to go somewhere else out of the bloodstream to prevent hyperglycemia (high blood sugar levels, like in a diabetic). It now gets stored in our fat tissue=fat or weight gain, again especially if you’re eating too high a quantity in your meals, or too high a quantity in starches, or even calories=sugars, or carbohydrates and even fats. All there ending product is in the blood after digestion in the stomach is sugar (simple or complex sugars). What will result in time from this type of dieting: you have high probability of becoming overweight to obese with cellulite developing over the body (particularly the pelvic region, abdomen, thighs and buttock). The degree of cellulite will depend on age factor since it will increase the probability for women in menopause), type of activity in that individual’s life- -moving from active to sedentary lifestyle, unhealthy eating to unhealthy habits over years vs healthy. The answer is not necessarily to perform a heavy workout including weights (especially if overweight or obese since the fat will turn to muscle and unless you do weight lifting till you die, like Jack Lanne, it will turn back to fat and cellulite). The key is living healthier habits, good dieting (6 small meals a day to balance your metabolism=sugar level), knowing the 4 food groups and how to dispense them in your meals properly (CHOs, sugars=calories,starches, and fats) and knowing what is in the liquids you drink (many with high sugar contents, as simple as soda, coke or Pepsi, and fruit juices). I’m not saying start diet soda (since it contains phenylalanine or NutraSweet both that can cause cancer) but water (plain or flavored) or club soda or certain ice teas or lemonades (particularly homemade) depending on the ingredients. You have to just read the ingredients to see that the sugar, CHO, calories, fat, and starch content is low with the protein higher than the rest. If you eat 6 meals a day the protein should be over 12.
The reason why cellulite is our enemy is because for it to even show up on the body you have to become overweight to obese. Obesity is a major enemy for any country to have in high population because of the diseases Obesity alone can cause. It can cause diabetes 2, high blood pressure, stroke, coronary artery disease, joint problems including osteoarthritis, metabolic syndrome, in women contributes to a variety of cancers including breast/colon/gallbladder/uterus, in men contributes to having a higher risk of colon or prostate cancers, sleep apnea and respiratory problems and could go on. Now do you see why developing cellulite is our enemy=Obesity and what it can cause alone.
Cellulite is something we can resolve by decreasing weight and having daily or at least every other day some activity from fast walking to jogging or even Pilates. If your disabled and can’t do much activity you surely can do something through your diet. To get started and if you need guidance on how to lose weight. This includes 6 meals a day with learning about the 4 groups (knowing from each group what’s lean, leaner, and leanest) to learning what activity does for the body then you came to the right blog. If you want to learn more about this than go to my website healthyusa.tsfl.com and peek at what we can offer you through Dr. Wayne Scott Anderson with his book “Dr A’s Habits of Health” and even foods to buy if you want them in the beginning of your diet loss which provides health bars to lunches and dinners to desserts of all kinds to all types of shakes/drinks and so much more foods (low in fat/calories/carbs/starches). Learn how to become healthier for yourself, even spreading the news to family or friends who may become interested and being a great mentor for your children in helping the next generation to be more healthy which would help our health care system to our health economy that includes insurance payments for bills at hospitals/doctor’s offices which would lessen. Our society has become so unhealthy in diet causing so many increases in diseases/illnesses, including children, (Obesity, Diabetes II, coronary artery disease, hypertension, and more) that we have the government getting involved. Take a look at Facebook or YouTube with pictures of people in America shopping at Walmart or Kmart. It may be funny to some people but it is also outright scary with what’s happening to our country. Our country has increased drastically in poor health habits that killed our economy, with let alone our health care system including what insurance costs are like for our society. We could, as a society, turn things around for the better regarding ourselves and others in our country for everyone’s health that would impact every American citizen of all ages in a positive way. I hope I have impacted someone in this country in wanting to learn more about knowing how to become healthier with making a good change for our country as a diversified whole. Society has a responsibility and impact on how things run in each of their respective countries but especially in America, since we live in a democracy. Its common sense if we get better regarding our health overall it will put an impact on our health economy if we don’t our health care system will just get WORSE. Do mom’s and dad’s want this for their children’s future or their grandchildren or even their own lives? Society has to take a stand, don’t leave it up to our government but leave it up to our citizens in America’s homes with our schools (Ex.proper health teaching regarding the cafeteria food), our restaurant industry (get off of living with such processed and fast foods in our states) and lastly our government to an extent. What does any politician really care, in having as a top priority being health since their getting top quality insurance and making high incomes to live life up (President Obama upon retirement will be the first President making 450,000 dollars a year). I know I would be a happy camper too if I was in that situation and I could go on with other politicians salaries but I started with the top. So let’s make a move America and go for the healthier aspect of life.