Treatments for CHF:
Heart failure caused by an excessive workload is curable by treating the primary disease, such as anemia or thyrotoxicosis or hypertension or diabetes. Also, curable are forms caused by anatomical problems such as a heart valve defect. These defects can be surgically corrected.
However, for the common forms of heart failure due to damaged heart muscle no known cure (like a heart attack that damages the heart muscle where the attack took place on the organ) but prevention of it happening again can take place in many cases through treatment of the disease or illness with being compliant in following up with your doctor for the disease or illness and being compliant in following doctor’s orders. The worst thing you can do is ignore them. The treatment seeks to improve patients quality of life and length of survival through lifestyle change and drug therapy.
Patients can minimize the effect of heart failure by controlling the risk factors for heart disease they may have. Obvious steps include: Don’t smoke or quit smoking, lose weight if necessary, abstaining from alcohol, making those dietary changes to reduce the amount of salt and fat consumed. Also, regular with modest exercise is also helpful for many patients; though the amount and intensity should be carefully monitored by a physician.
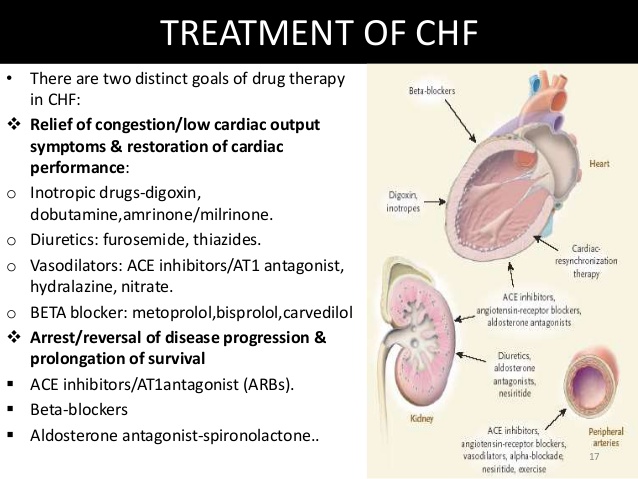
Even with lifestyle changes, most heart failure patients must take medication. Many patients receive 2 or more meds. Types of common medications given are: ACE inhibitors, Digitalis, Diuretics, Hydralazine, and Nitrates.
These are some of the meds given for heart failure. Not all medications are suitable for patients, and more than one drug may be needed. Always review the list your pharmacist provides in the action, side effects, with instructions of how to take the drug to make it most effective in your body with what to look for while on this medication to keep you the patient most informed on what you should be aware of since your on the medication. You should know what your taking.
Results of studies over the years have placed more emphasis on the use of drugs known as angiotensin converting enzymes (ACE) inhibitors. Several studies have indicated that ACE inhibitors improve survival among heart failure patients and may slow perhaps even prevent the loss of the heart pumping activity. This drug prevents the transfer of your enzyme Angiotensin 1 to convert into Angiotensin 2 which prevents the vessels in your body to do vasoconstriction which prevents the pressure in the bloodstream to raise = high B/P (hypertension) but this medication prevents this from happening. By the medication doing this it prevents stress to the heart; with vasoconstriction in causing the B/P to go high this now causes the blood to get to the heart slowly and more difficult causing the heart to pump harder but the ACE inhibitor with allowing vasodilation (opening of vessels) keeps the pressure down to make the job easier= less stress on the heart. Originally these medications where for patients in the treatment of hypertension but they help patients with heart failure, among other things, decreasing the pressure inside the blood vessels causing the heart to do its job easier.
Digitalis increases the force of the heart’s contractions, helping to improve circulation in the body.
Diuretics are for reducing the amount of fluid in the bloodstream and body by releasing them via the kidneys and having us void the excess of water out in our urine, these are useful for patients with fluid retention.
Those who aren’t prescribed or cannot take these meds already mentioned may be given a hydralazine medication and/or a drug in the Nitrate classification, each of which help relax tension in the blood vessels to improve blood flow. Also, both Hydralazine and Nitrates function is they cause vasodilation in the vessels improving blood flow to the heart.
Sometimes heart failure is life threatening. Usually, this happens when drug therapy and lifestyle changes fail to control its symptoms. In such cases, a heart transplant may be the only treatment option. However, candidates for transplantation often have to wait months or even years before a suitable donor heart is found.
Studies over the years indicate that some transplant candidates improve during this waiting period through drug treatment and other therapy, and can be removed from the transplant list.
Transplant candidates who do not improve sometimes need mechanical pumps, which are attached to the heart. Called left ventricular assist device (LVADs), the machine takes over part or virtually all of the heart’s blood-pumping activity. However, current LVADs are not permanent solutions for heart failure but are considered bridges to transplantation. Worldwide, about 3,500 heart transplants were performed annually. The vast majority of these are performed in the United States (2,000-2,300 annually). Cedars Sinai Medical Center in Los Angeles, California has performed the most heart transplants in the last three consecutive years performing 95 transplants in 2012 alone. About 800,000 people have a Class IV heart defect indicating a new organ. The degrees of CHF are I, II, III and IV. In learning more about CHF with heart transplants (including becoming a candidate for one) go to wwwtransplantexperience.com or even hearttransplant.com.
Another surgical procedure for heart failure that is available in America is cardiomyoplasty. This is a surgical procedure in which healthy muscle from another part of the body is wrapped around the heart to provide support for the failing heart. A special pacemaker is implanted to make the skeletal muscle contract.
Complications of CHF:
Through the Mayo clinic as a reference regarding complications their website stated: “If you have heart failure, your outlook depends on the cause and the severity, your overall health, and other factors such as your age. Complications can include:
- Kidney damage or failure. Heart failure can reduce the blood flow to your kidneys, which can eventually cause kidney failure if left untreated. Kidney damage from heart failure can require dialysis for treatment.
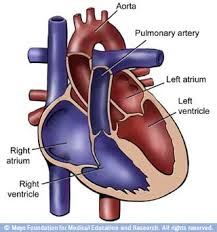
- Heart valve problems. The valves of your heart, which keep blood flowing in the proper direction through your heart, may not function properly if your heart is enlarged, or if the pressure in your heart is very high due to heart failure.
- Liver damage. Heart failure can lead to a buildup of fluid that puts too much pressure on the liver. This fluid backup can lead to scarring, which makes it more difficult for your liver to function properly.
- Stroke. Because blood flow through the heart is slower in heart failure than in a normal heart, it’s more likely you’ll develop blood clots, which can increase your risk of having a stroke.Tips on CHF:Closely follow your doctor’s instructions, being compliant with the instructions and taking your meds.Control your weight in making it easier for your heart, that’s in failure, to function better (less stress).Limit or stop alcohol consumption as your doctor informs you.The best defense against heart failure is PREVENTION! Almost all the cardiac risk factors can be controlled by eliminating the bad unhealthy habits (smoking, obese, high cholesterol, high B/P, diabetes).
- Going to the doctor can be stressful but know he is there for you. It is hard to remember everything you want to ask the doctor with everything you hear at your visit. It helps to prepare a list of questions you may have and bring it with you at your appointment to address to the concerns you listed to the doctor. In doing this it helps you with your appointment so you can record the answers by listing them on the paper you have. Before you leave the doctor’s office, be sure you understand your condition, its treatment, including any medications your taking this doctor that he or sheprescribed for you with that doctor knowing any other medications you may be on through a different doctor to prevent side effects or adverse reactions occurring but if you forget this about the medications there is always your pharmacist you can ask, than your personal M.D. later. With you knowing all this information you will see why it is so vital for you doing all these actions or interventions for your disease that your doctor prescribed or ordered and you’re more out to follow them as well with understanding the whole picture about the treatment for CHF.
- Of course, stop smoking permanently if actively smoking.
- Watch what you eat and how much. Watch the diet intake of cholesterol and sodium that can cause a negative impact on the heart by causing stress to the organ through either high B/P=high sodium intake that causes vasoconstriction or high cholesterol intake frequently that commonly causes blockage in an artery. Both high sodium or high cholesterol cause diminishing of oxygenated blood getting to the heart. Without oxygen to our tissues or cells this causes tissue & cellular starvation (ischemia). What is starvation to the heart=ischemia to the heart=chest pain (what we call angina). Take a brittle diabetic, the furthest area from the heart is the feet the first area to experience starvation is the toes, foot or lower extremity which is why this is usually the first to be amputated if necessary (you usually see an upper extremity amputated due to trauma not disease).
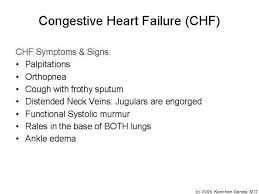
- Immediately call your doctor of any significant change in your condition, such as an intensified shortness of breath or swollen feet or weight gain of 3lbs or more within one week.
- See your doctor regularly in evaluating your CHF.
- Some people’s symptoms and heart function will improve with proper treatment. However, heart failure can be life-threatening. People with heart failure may have severe symptoms, and some may require heart transplantation or support with an artificial heart device.”
If you are needing any guidance in how to lose weight through using all 4 food groups, with assistance in what to eat now to lose weight till you are in therapeutic range for your height rather than eating food from the market or if you need to understand how the body works with food and metabolism with where activity comes into play go to healthyusa.tsfl.com. See what we can provide you in answering all these questions for you through Dr. Anderson and myself as your coach free. SO LIVE AS HEALTHY AS POSSIBLE IN YOUR ROUTINE HABITS, YOUR DIETING OF THE 4 FOOD GROUPS, MAINTAINING YOUR WEIGHT IN A THEREPEUTIC RANGE (look as calculating BMI online for free to find out what your weight range for your height is), and BALANCING REST WITH EXERCISE TO HELP DECREASE THE CHANCE OF GETTING HEART FAILURE. Join me like many who are trying to live life healthier with making America a healthier home and we all should take part to help the health care system to be more effective for our society. Recommended to anyone with disease before changing your diet, activity/exercise program review your changes with your doctor to get clearance first to maintain your safety.
We can fulfill this goal, the one step America is by getting healthier (through diet, exercise, and living healthier habits) which would impact cardiac disease by decreasing it in time which would decrease congestive heart failure. Learn more about CHF on striveforgoodhealth.com with learning how to reach this goal. Let us the people of America take part on decreasing disease and not just leave it the health care or government’s hands. Look at the results already and we the society need to take be responsible in being better for ourselves, our children and our future generations.