Archives
QUOTE FOR TUESDAY:
“Some of the diseases that can cause symptoms of dementia include alzheimer’s disease (AD).
They also lose their ability to solve problems and maintain emotional control, and they may experience personality changes and behavioral problems, such as agitation, delusions, and hallucinations. While memory loss is a common symptom of dementia, memory loss by itself does not mean that a person has dementia. Doctors diagnose dementia only if two or more brain functions – such as memory and language skills — are significantly impaired without loss of consciousness.
Moreover, recent studies have found that newer brain scans may point to other causes of Dementia in approximately one-third of presumed AD cases, thereby helping avoid an Alzheimer’s disease misdiagnosis, which may lead to better treatment and care.**
A fundamental concept to grasp is that the symptoms of Dementia often go beyond memory loss. They can include significant shifts in mood, more falls, disturbed gait (how we walk), and more. In addition, hallucinations, delusions, and paranoia are not uncommon.”
Dementia Society of America (Dementia Society of America® | Definitions)
Part IV Alzheimer’s Disease – Tips for preventing Alzheimer’s Disease!

More Tips for Avoiding Alzheimer’s Disease:
The beauty of following a healthy diet is that it helps treat and prevent all chronic degenerative diseases, from the common ones like heart disease, cancer, diabetes, obesity and Alzheimer’s to the ones you have never heard of or can’t even pronounce.
The first step is to eat healthy, maintaining exercise balanced with rest and practice healthy habits in addressing Alzheimer’s disease, which is currently at epidemic proportions, with 5.4 million Americans – including one in eight people aged 65 and over – living with the disease.By 2050, this is expected to jump to 16 million, and in the next 20 years it is projected that Alzheimer’s will affect one in four Americans. People we need to live healthier if not to help ourselves our future young ones.
In spite of how common memory loss is among Westerners, it is NOT a “normal” part of aging. While even mild “senior moments” may be caused by the same brain lesions associated with Alzheimer’s disease and other forms of dementia, these cognitive changes are by no means inevitable! People who experience very little decline in their cognitive function up until their deaths have been found (post-mortem) to be free of brain lesions, showing that it’s entirely possible to prevent the damage from occurring in the first place and one of the best ways to do this is by leading a healthy lifestyle.
-
Fructose. As mentioned, most everyone will benefit from keeping their total fructose consumed to below 25 grams per day.
-
Improve Magnesium Levels. There is some exciting preliminary research strongly suggesting a decrease in Alzheimer symptoms with increased levels of magnesium in the brain. Unfortunately most magnesium supplements do not pass the blood brain levels, but a new one, magnesium threonate, appears to and holds some promise for the future for treating this condition.
-
Optimize your vitamin D levels with safe sun exposure. Strong links between low levels of vitamin D in Alzheimer’s patients and poor outcomes on cognitive tests have been revealed. Researchers believe that optimal vitamin D levels may enhance the amount of important chemicals in your brain and protect brain cells by increasing the effectiveness of the glial cells in nursing damaged neurons back to health.
-
Vitamin D may also exert some of its beneficial effects on Alzheimer’s through its anti-inflammatory and immune-boosting properties. Sufficient vitamin D is imperative for proper functioning of your immune system to combat inflammation that is also associated with Alzheimer’s.
-
Vitamin B12: According to a small Finnish study recently published in the journal Neurology, people who consume foods rich in B12 may reduce their risk of Alzheimer’s in their later years. For each unit increase in the marker of vitamin B12 (holotranscobalamin) the risk of developing Alzheimer’s was reduced by 2 percent. Very high doses of B vitamins have also been found to treat Alzheimer’s disease and reduce memory loss.
-
Eat a nutritious diet, rich in folate. Vegetables, without question, are your best form of folate, and we should all eat plenty of fresh raw veggies every day.
-
High-quality animal-based omega-3 fats, such as krill oil. (I recommend avoiding most fish because, although fish is naturally high in omega-3, most fish are now severely contaminated with mercury.) High intake of the omega-3 fats EPA and DHA help by preventing cell damage caused by Alzheimer’s disease, thereby slowing down its progression, and lowering your risk of developing the disorder.
-
Avoid and remove mercury from your body. Dental amalgam fillings, which are 50% mercury by weight, are one of the major sources of heavy metal toxicity, however you should be healthy prior to having them removed.
-
Avoid aluminum, such as antiperspirants, non-stick cookware, vaccine adjuvants, etc.
-
Exercise regularly. It’s been suggested that exercise can trigger a change in the way the amyloid precursor protein is metabolized,10 thus, slowing down the onset and progression of Alzheimer’s. Exercise also increases levels of the protein PGC-1alpha. Research has also shown that people with Alzheimer’s have less PGC-1alpha in their brains11 and cells that contain more of the protein produce less of the toxic amyloid protein associated with Alzheimer’s. I would strongly recommend reviewing the Peak Fitness Technique for my specific recommendations.
-
Avoid flu vaccinations as most contain both mercury and aluminum, well-known neurotoxic and immunotoxic agents.
-
Eat plenty of blueberries. Wild blueberries, which have high anthocyanin and antioxidant content, are known to guard against Alzheimer’s and other neurological diseases.
-
Challenge your mind daily. Mental stimulation, especially learning something new, such as learning to play an instrument or a new language, is associated with a decreased risk of Alzheimer’s. Researchers suspect that mental challenge helps to build up your brain, making it less susceptible to the lesions associated with Alzheimer’s disease.
-
Avoid anticholinergic and statin drugs. Drugs that block acetylcholine, a nervous system neurotransmitter, have been shown to increase your risk of dementia. These drugs include certain nighttime pain relievers, antihistamines, sleep aids, certain antidepressants, medications to control incontinence, and certain narcotic pain relievers.
-
Statin drugs are particularly problematic because they suppress the synthesis of cholesterol, deplete your brain of coenzyme Q10 and neurotransmitter precursors, and prevent adequate delivery of essential fatty acids and fat-soluble antioxidants to your brain by inhibiting the production of the indispensable carrier biomolecule known as low-density lipoprotein.
** Before making any changes check with your primary care doctor or neurologist first.**
QUOTE FOR MONDAY:
“Over 55 million people around the world live with dementia, and as the global population ages, that number is expected to nearly triple by 2050. Alzheimer’s disease, the most common form of dementia, accounting for an estimated 60 to 70% of cases, is a neurodegenerative disorder characterized by the accumulation of amyloid plaques and tau neurofibrillary tangles that leads to memory loss and a decline in cognitive abilities so significant, it interferes with daily life and ultimately results in death.
For more than three decades, Johnson & Johnson scientists have been working to better understand the complex biology of Alzheimer’s disease and pioneer new ways to treat it. Today, it’s recognized as a progressive continuum that begins silently with the accumulation of amyloid and tau in the brain, often years before symptoms appear. ”
Now, the company is closer than ever to reaching three significant goals in the fight against Alzheimer’s disease.”
*Both Plaques and Tangles are present in the brains of individuals without Alzheimer’s; however, they are found at much higher levels in the brains of Alzheimer’s patients.
It is theorized that the root causes of Alzheimer’s disease are the factors which control the amount of Amyloid and Tau in the brain. Factors like the ApoE gene. These are 2 plaques damaging brain cells and cause the brain lesions characteristic of Alzheimer’s disease.*
Johnson and Johnson (How J&J is advancing the fight against Alzheimer’s disease )
Part III Alzheimer’s Disease – Learn some facts and causes of this diagnosis!!
People with this disease:
- In 2014, as many as 5 million Americans were living with Alzheimer’s disease.
- The symptoms of the disease can first appear after age 60 and the risk increases with age.
- Younger people may get Alzheimer’s disease, but it is less common.
- The number of people living with the disease doubles every 5 years beyond age 65.
- This number is projected to nearly triple to 14 million people by 2060.
Scientists do not yet fully understand what causes Alzheimer’s disease. There probably is not one single cause, but several factors that affect each person differently.
- Age is the best known risk factor for Alzheimer’s disease.
- Family history—researchers believe that genetics may play a role in developing Alzheimer’s disease.
- Changes in the brain can begin years before the first symptoms appear.
- Researchers are studying whether education, diet, and environment play a role in developing Alzheimer’s disease.
- Scientists are finding more evidence that some of the risk factors for heart disease and stroke, such as high blood pressure and high cholesterol may also increase the risk of Alzheimer’s disease.
- There is growing evidence that physical, mental, and social activities may reduce the risk of Alzheimer’s disease.
Alzheimer’s disease is
- One of the top 10 leading causes of death in the United States.
- The 6th leading cause of death among US adults.
- The 5th leading cause of death among adults aged 65 years or older.
In 2014, an estimated 5 million Americans aged 65 years or older had Alzheimer’s disease. This number is projected to nearly triple to 14 million people by 2060.
In 2010, the costs of treating Alzheimer’s disease were projected to fall between $159 and $215 billion.4 By 2040, these costs are projected to jump to between $379 and more than $500 billion annually.4
Death rates for Alzheimer’s disease are increasing, unlike heart disease and cancer death rates that are on the decline.5 Dementia, including Alzheimer’s disease, has been shown to be under-reported in death certificates and therefore the proportion of older people who die from Alzheimer’s may be considerably higher.
Various disorders and factors contribute to the development of dementia. Neuro-degenerative disorders result in a progressive and irreversible loss of neurons and brain functioning. Currently, there are no cures for these types of disorders. They include:
Other types of progressive brain disease include:
- Vascular contributions to cognitive impairment and dementia
- Mixed dementia, a combination of two or more types of dementia
In addition, certain medical conditions can cause serious memory problems that resemble dementia. These problems should go away once the conditions are treated. These conditions include:
- Side effects of certain medicines
- Emotional problems, such as stress, anxiety, or depression
- Certain vitamin deficiencies
- Drinking too much alcohol
- Blood clots, tumors, or infections in the brain
- Delirium
- Head injury, such as a concussion from a fall or accident
- Thyroid, kidney, or liver problems
Doctors have identified many other conditions that can cause dementia or dementia-like symptoms. These conditions include:
- Argyrophilic grain disease, a common, late-onset degenerative disease
- Creutzfeldt-Jakob disease, a rare brain disorder
- Huntington’s disease, an inherited, progressive brain disease
- Chronic traumatic encephalopathy (CTE), caused by repeated traumatic brain injury
- HIV-associated dementia (HAD)
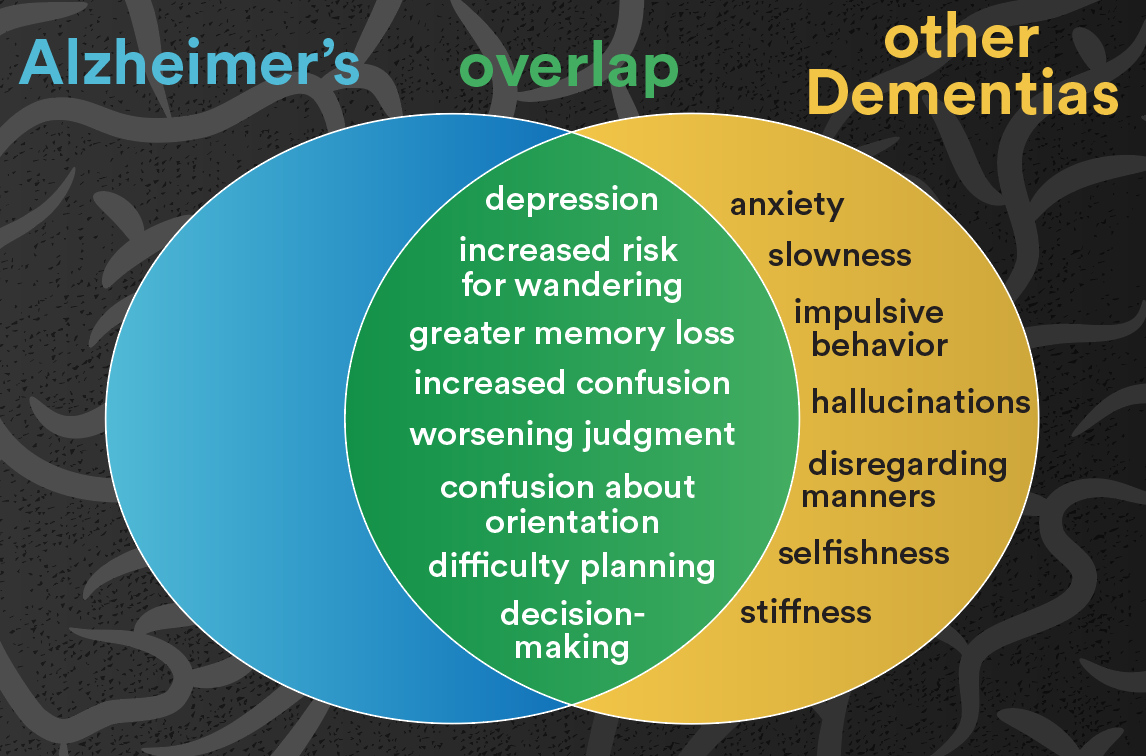
The overlap in symptoms of various dementias can make it hard to get an accurate diagnosis. But a proper diagnosis is important to get the right treatment. Seek help from a neurologist—a doctor who specializes in disorders of the brain and nervous system—or other medical specialist who knows about dementia.
QUOTE FOR THE WEEKEND:
“Early symptoms of Alzheimer’s disease include forgetting recent events or conversations. Over time, Alzheimer’s disease leads to serious memory loss and affects a person’s ability to do everyday tasks.
There is no cure for Alzheimer’s disease. In advanced stages, loss of brain function can cause dehydration, poor nutrition or infection. These complications can result in death.
But medicines may improve symptoms or slow the decline in thinking. Programs and services can help support people with the disease and their caregivers.”
MAYO CLINIC (Alzheimer’s disease – Symptoms and causes – Mayo Clinic)
Part II Alzheimer’s Disease Awareness – diagnosing and treatment.


The National Institute of aging states the following procedures also may be used to diagnose dementia:
- “Cognitive and neuropsychological tests. These tests are used to assess memory, problem solving, language skills, math skills, and other abilities related to mental functioning.
- Laboratory tests. Testing a person’s blood and other fluids , as well as checking levels of various chemicals, hormones, and vitamins, can help find or rule out possible causes of symptoms.
- Brain scans. These tests can identify strokes, tumors, and other problems that can cause dementia. Scans also identify changes in the brain’s structure and function. The most common scans are:
- Computed tomography (CT), which uses x rays to produce images of the brain and other organs
- Magnetic resonance imaging (MRI), which uses magnetic fields and radio waves to produce detailed images of body structures, including tissues, organs, bones, and nerves
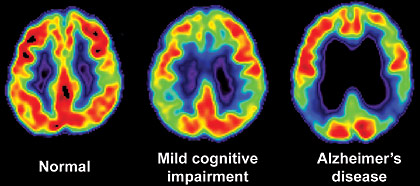
- Positron emission tomography (PET), which uses radiation to provide pictures of brain activity
- Psychiatric evaluation. This evaluation will help determine if depression or another mental health condition is causing or contributing to a person’s symptoms.
- Genetic tests. Some dementias are caused by a known gene defect. In these cases, a genetic test can help people know if they are at risk for dementia. It is important to talk with a genetic counselor before and after getting tested, along with family members and the doctor.
QUOTE FOR FRIDAY:
“Dementia is a general term for loss of memory, language, problem-solving and other thinking abilities that are severe enough to interfere with daily life. Alzheimer’s is the most common cause of dementia.
Some risk factors for dementia, such as age and genetics, cannot be changed. But researchers continue to explore the impact of other risk factors on brain health and prevention of dementia.
Protecting your brain health — how well you think, learn and remember — is important at every age. Building brain-healthy habits can help you live better now and protect your memory and thinking for the future. Brain health is important for everyone, including people with a family history of dementia. It is never too early or too late to take action for your brain health.”
Alzheimer’s Association (What is Dementia? Symptoms, Causes & Treatment | alz.org)
Part I What is actually Alzheimer’s Disease & the symptoms?
What structurally happens to the brain and what happens to the individual in brain thinking diagnosed with this disease:
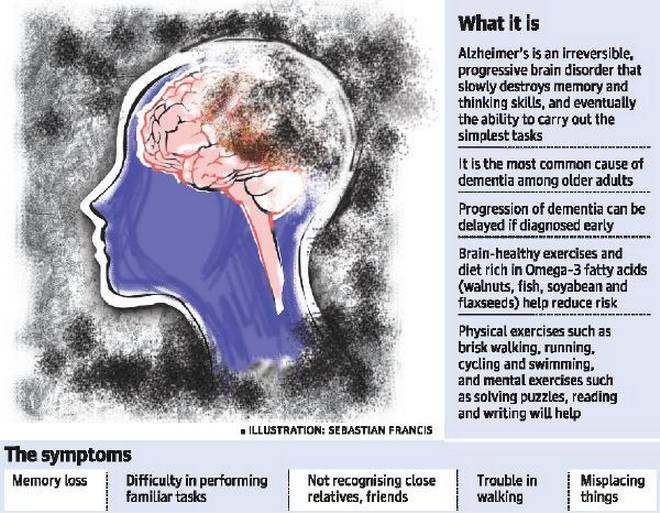
Alzheimer’s disease is an irreversible, progressive brain disorder that slowly destroys memory and thinking skills and, eventually, the ability to carry out the simplest tasks. In most people with the disease—those with the late-onset type—symptoms first appear in their mid-60s. Early-onset Alzheimer’s occurs between a person’s 30s and mid-60s and is very rare. Alzheimer’s disease is the most common cause of dementia among older adults.
The disease is named after Dr. Alois Alzheimer. In 1906, Dr. Alzheimer noticed changes in the brain tissue of a woman who had died of an unusual mental illness. Her symptoms included memory loss, language problems, and unpredictable behavior. After she died, he examined her brain and found many abnormal clumps (now called amyloid plaques) and tangled bundles of fibers (now called neurofibrillary, or tau, tangles).
These plaques and tangles in the brain are still considered some of the main features of Alzheimer’s disease. Another feature is the loss of connections between nerve cells (neurons) in the brain. Neurons transmit messages between different parts of the brain, and from the brain to muscles and organs in the body. Many other complex brain changes are thought to play a role in Alzheimer’s, too.
This damage initially appears to take place in the hippocampus, the part of the brain essential in forming memories. As neurons die, additional parts of the brain are affected. By the final stage of Alzheimer’s, damage is widespread, and brain tissue has shrunk significantly.
How many affected in the United States by Alzheimer’s Disease:
Estimates vary, but experts suggest that as many as 5.5 million Americans age 65 and older may have Alzheimer’s. Many more under age 65 also have the disease. Unless Alzheimer’s can be effectively treated or prevented, the number of people with it will increase significantly if current population trends continue. This is because increasing age is the most important known risk factor for Alzheimer’s disease.
Symptoms:
Memory problems are typically one of the first signs of Alzheimer’s, though initial symptoms may vary from person to person. A decline in other aspects of thinking, such as finding the right words, vision/spatial issues, and impaired reasoning or judgment, may also signal the very early stages of Alzheimer’s disease. Mild cognitive impairment (MCI) is a condition that can be an early sign of Alzheimer’s, but not everyone with MCI will develop the disease.
People with Alzheimer’s have trouble doing everyday things like driving a car, cooking a meal, or paying bills. They may ask the same questions over and over, get lost easily, lose things or put them in odd places, and find even simple things confusing. As the disease progresses, some people become worried, angry, or violent.
Alzheimer’s disease is not a normal part of aging.
Memory problems are typically one of the first warning signs of cognitive loss.
According to the National Institute on Aging, in addition to memory problems, someone with Alzheimer’s disease may experience one or more of the following signs:
- Memory loss that disrupts daily life, such as getting lost in a familiar place or repeating questions.
- Trouble handling money and paying bills.
- Difficulty completing familiar tasks at home, at work or at leisure.
- Decreased or poor judgment.
- Misplaces things and being unable to retrace steps to find them.
- Changes in mood, personality, or behavioral.
QUOTE FOR THURSDAY:
“How common is pancreatic cancer?
The American Cancer Society’s estimates for pancreatic cancer in the United States for 2025 are:
- About 67,440 people ( 34,950 men and 32,490 women) will be diagnosed with pancreatic cancer.
- About 51,980 people ( 27,050 men and 24,930 women) will die of pancreatic cancer.
Lifetime risk of pancreatic cancer
The average lifetime risk of pancreatic cancer is about 1 in 56 in men and about 1 in 60 in women. But each person’s chances of getting this cancer can be affected by certain risk factors.”
American Cancer Society (Facts About Pancreatic Cancer | American Cancer Society)