Virginia Postrel (born January 14, 1960 is an American political and a cultural writer).
Archives
Kidneys anatomy and functions to understand what happens with kidney failure!
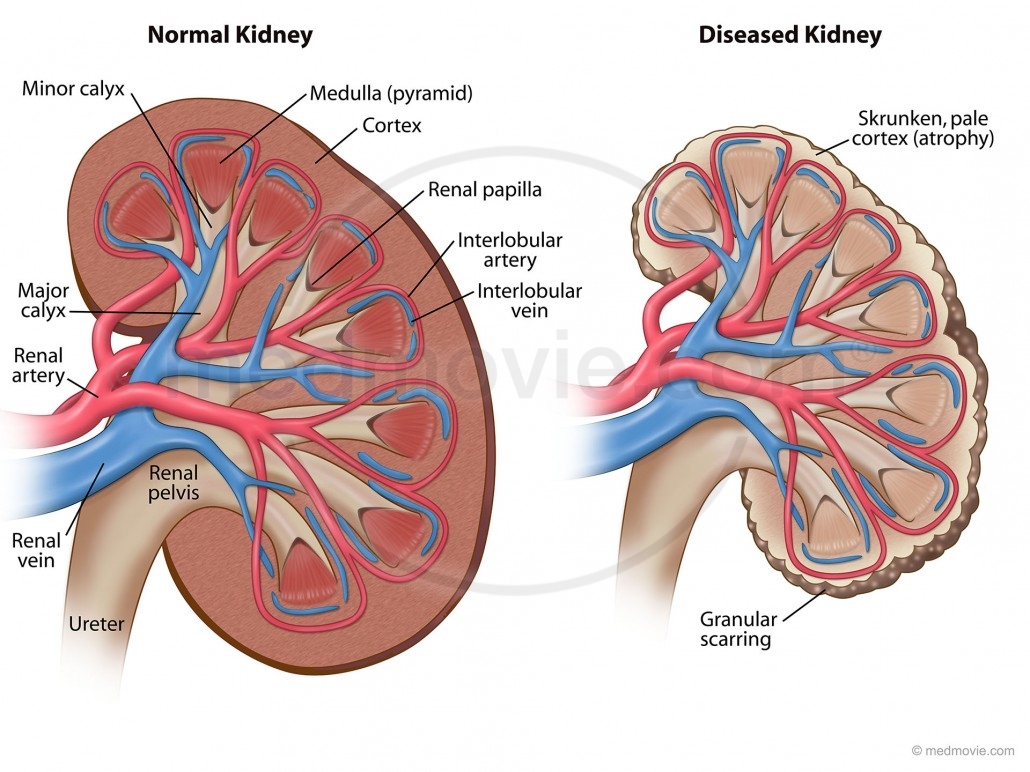
The kidneys are important organs with many functions in the body, including producing hormones, absorbing minerals, and filtering blood and producing urine. While they are important and kidney failure can be fatal, a human only needs one healthy kidney to survive.
The kidneys are two bean-shaped organs that extract waste from blood, balance body fluids, form urine, and aid in other important functions of the body.
They reside against the back muscles in the upper abdominal cavity. They sit opposite each other on either side of the spine. The right kidney sits a little bit lower than the left to accommodate the liver.
When it comes to components of the urinary system, the kidneys are multi-functional powerhouses of activity, for if the kidneys aren’t working, meaning they don’t filter toxic wastes out of our blood stream (with other functions it does) than the waste products don’t get dumped into the urinary bladder from the renal tubes, called right and left ureters. In human anatomy, the ureters are tubes made of smooth muscle fibers that propel urine from the kidneys to the urinary bladder. If the kidneys are not working they are not filtering our blood (same principle as filtering beer to make it to perfection, the kidneys do it for our blood to be able to have the cells do their function to the optimal levels with keeping toxins out of the body in preventing many blood problems with more due to acidosis (toxin build up). In the adult, the ureters are usually 25–30 cm (10–12 in) long and ~3–4 mm in diameter.
The kidneys have multiple functions. Some of the core actions of a healthy kidney or kidneys of a human body include:
- Waste excretion: There are many things your body doesn’t want inside of it. The kidneys filter out toxins, excess salts, and urea (a toxin), a nitrogen-based waste created by cell metabolism. * Urea is an organic chemical compound and is essentially the waste produced by the body after metabolizing protein. Naturally the compound urea is produced when the liver breaks down protein or amino acids, and ammonia, the kidneys then transfer the urea from the blood to the urine, when they do filtering of the blood. * Urea is a byproduct of protein metabolism, the ending result. *Extra nitrogen is expelled from the body through urea because it is extremely soluble (solid); it is a very efficient process. The average person excretes about 30 grams of urea a day, mostly through urine but a small amount is also secreted in perspiration. Synthetic versions of the chemical compound can be created in liquid or solid form and is often an ingredient found in fertilizers, animal food, and diuretics, just to name a few . Urea is what gives our urine the color yellow. *In the gastrointestinal tract, blood proteins are broken down into ammonia (could be due to high protein eating to drugs with actual conditions); and goes to the liver converting it to Urea. It is then released into the blood stream where the kidney’s take it up and eliminate it. Urea is then eliminated by the kidney’s, but not produced by it. *Urea is synthesized in the liver and transported through the blood to the kidneys for removal.
- A Healthy Kidney or Kidneys functions in the human body:
- Water level balancing: As the kidneys are key in the chemical breakdown of urine, they react to changes in the body’s water level throughout the day. As water intake decreases, the kidneys adjust accordingly and leave water in the body instead of helping excrete it which aides in electrolyte balancing in the blood with keeping the body hydrated properly.
- Blood pressure regulation: The kidneys need constant pressure to filter the blood. When it drops too low, the kidneys increase the pressure. One way is by producing a blood vessel-constricting protein (angiotensin) that also signals the body to retain sodium and water. Both the constriction and retention help restore normal blood pressure.
- Red blood cell regulation: When the kidneys don’t get enough oxygen, they send out a distress call in the form of erythropoietin, a hormone that stimulates the bone marrow to produce more oxygen-carrying red blood cells.
- Acid regulation: As cells metabolize, they produce acids. Foods we eat can either increase the acid in our body or neutralize it. If the body is to function properly, it needs to keep a healthy balance of these chemicals. The kidneys do that, too.Because of all of the vital functions the kidneys perform and the toxins they encounter, the kidneys are susceptible to various problems.
- Acute kidney failure is a condition in which the kidneys suddenly lose their ability to function properly. This can occur for many reasons, including:
- Most people are born with two kidneys, but many people can live on just one. Kidney transplant surgeries with live donors are common medical procedures today.
- Infection
- Blood-clotting disorders
- Decreased blood flow caused by low blood pressure
- Autoimmune kidney disorders
- Urinary tract infections
- Complications from pregnancy
- DehydrationDiseases and conditions that commonly cause chronic kidney disease include:
- Chronic kidney failure – same as acute in that the kidney (s) loses its function.
- Type 1 or type 2 diabetes
- High blood pressure
- Glomerulonephritis (gloe-mer-u-lo-nuh-FRY-tis), an inflammation of the kidney’s filtering units (glomeruli)
- Interstitial nephritis, an inflammation of the kidney’s tubules and surrounding structures
- Polycystic kidney disease
- Prolonged obstruction of the urinary tract, from conditions such as enlarged prostate, kidney stones and some cancers
- Vesicoureteral (ves-ih-koe-yoo-REE-ter-ul) reflux, a condition that causes urine to back up into your kidneys
- Recurrent kidney infection, also called pyelonephritis (pie-uh-lo-nuh-FRY-tis)
- A chronic condition causes the failure to happen, what we call a secondary diagnosis. * Learn more tomorrow, on Thursday, about Acute and Chronic kidney failure.
QUOTE FOR TUESDAY:
“I would not have traded two minutes of the joy and the grief with that man for two decades of anything with another.”
– Lou Gehrig’s wife, Eleanor
Lou Gehrigs Disease=Amyotrophic lateral sclerosis
ALS, or amyotrophic lateral sclerosis, is a progressive neurodegenerative disease that affects nerve cells in the brain and the spinal cord. A-myo-trophic comes from the Greek language. “A” means no. “Myo” refers to muscle, and “Trophic” means nourishment – “No muscle nourishment.” When a muscle has no nourishment, it “atrophies” or wastes away. “Lateral” identifies the areas in a person’s spinal cord where portions of the nerve cells that signal and control the muscles are located. As this area degenerates it leads to scarring or hardening (“sclerosis”) in the region.
Motor neurons reach from the brain to the spinal cord and from the spinal cord to the muscles throughout the body. The progressive degeneration of the motor neurons in ALS eventually leads to their demise. When the motor neurons die, the ability of the brain to initiate and control muscle movement is lost. With voluntary muscle action progressively affected, people may lose the ability to speak, eat, move and breathe. The motor nerves that are affected when you have ALS are the motor neurons that provide voluntary movements and muscle control. Examples of voluntary movements are making the effort to reach for a smart phone or step off a curb. These actions are controlled by the muscles in the arms and legs. Motor neurons are nerve cells located in the brain, brain stem, and spinal cord that serve as controlling units and vital communication links between the nervous system and the voluntary muscles of the body. Messages from motor neurons in the brain called upper motor neurons are transmitted to motor neurons in the spinal cord which are lower motor neurons and from them to particular muscles. The problem with ACL, both the upper motor niurons and the ower motor niurons degenerate or die which causes stoppage of sending messages to muscles. Unable to function, the muscles gradually weaken, waste away (atrophy), and have very fine twitches (called fasciculations). Eventually, the ability of the brain to start voluntary movement with messages is unable to work anymore.
Symptoms:
The onset of ALS may be so subtle that the symptoms are overlooked. The earliest symptoms may include fasciculations, cramps, tight and stiff muscles (spasticity), muscle weakness affecting an arm or a leg, slurred and nasal speech, or difficulty chewing or swallowing. These general complaints then develop into more obvious weakness or atrophy that may cause a physician to suspect ALS. Regardless of the part of the body first affected by the disease, muscle weakness and atrophy spread to other parts of the body as the disease progresses.
The parts of the body showing early symptoms of ALS depend on which muscles in the body are affected. Many individuals first see the effects of the disease in a hand or arm as they experience difficulty with simple tasks requiring manual dexterity such as buttoning a shirt, writing, or turning a key in a lock. In other cases, symptoms initially affect one of the legs, and people experience awkwardness when walking or running or they notice that they are tripping or stumbling more often.
There are two different types of ALS, sporadic and familial. Sporadic which is the most common form of the disease in the U.S., is 90 – 95 percent of all cases. It may affect anyone, anywhere. Familial ALS (FALS) accounts for 5 to 10 percent of all cases in the U.S. Familial ALS means the disease is inherited. In those families, there is a 50% chance each offspring will inherit the gene mutation and may develop the disease. French neurologist Jean-Martin Charcot discovered the disease in 1869.
The cause of ALS is not known, and scientists do not yet know why ALS strikes some people and not others. An important step toward answering this question was made in 1993 when scientists supported by the National Institute of Neurological Disorders and Stroke (NINDS) discovered that mutations in the gene that produces the SOD1 enzyme were associated with some cases of familial ALS.
Recent years have brought a wealth of new scientific understanding regarding the physiology of this disease. There is currently one FDA approved drug, riluzole, that modestly slows the progression of ALS in some people. Although there is not yet a cure or treatment that halts or reverses ALS, scientists have made significant progress in learning more about this disease. In addition, people with ALS may experience a better quality of life in living with the disease by participating in support groups and attending an ALS Association Certified Treatment Center of Excellence or a Recognized Treatment Center. Such Centers provide a national standard of best-practice multidisciplinary care to help manage the symptoms of the disease and assist people living with ALS to maintain as much independence as possible for as long as possible. According to the American Academy of Neurology’s Practice Paramater Update, studies have shown that participation in a multidisciplinary ALS clinic may prolong survival and improve quality of life. To find a Center near you, visit http://www.alsa.org/community/certified-centers/.
ALS usually strikes people between the ages of 40 and 70, and approximately 20,000 Americans can have the disease at any given time (although this number fluctuates). For unknown reasons, military veterans are approximately twice as likely to be diagnosed with the disease than the general public. Notable individuals who have been diagnosed with ALS include baseball great Lou Gehrig, Hall of Fame pitcher Jim “Catfish” Hunter, Toto bassist Mike Porcaro, Senator Jacob Javits, actor David Niven, “Sesame Street” creator Jon Stone, boxing champion Ezzard Charles, NBA Hall of Fame basketball player George Yardley, golf caddie Bruce Edwards, , musician Lead Belly (Huddie Ledbetter), photographer Eddie Adams, entertainer Dennis Day, jazz musician Charles Mingus, former vice president of the United States Henry A. Wallace, U.S. Army General Maxwell Taylor, and NFL football players Steve Gleason, O.J. Brigance and Tim Shaw.
Who gets ALS?
More than 12,000 people in the U.S. have a definite diagnosis of ALS, for a prevalence of 3.9 cases per 100,000 persons in the U.S. general population, according to a report on data from the National ALS Registry. ALS is one of the most common neuromuscular diseases worldwide, and people of all races and ethnic backgrounds are affected. ALS is more common among white males, non-Hispanics, and persons aged 60–69 years, but younger and older people also can develop the disease. Men are affected more often than women.
In 90 to 95 percent of all ALS cases, the disease occurs apparently at random with no clearly associated risk factors. Individuals with this sporadic form of the disease do not have a family history of ALS, and their family members are not considered to be at increased risk for developing it.
About 5 to 10 percent of all ALS cases are inherited. The familial form of ALS usually results from a pattern of inheritance that requires only one parent to carry the gene responsible for the disease. Mutations in more than a dozen genes have been found to cause familial ALS.
About one-third of all familial cases (and a small percentage of sporadic cases) result from a defect in a gene known as “chromosome 9 open reading frame 72,” or C9orf72. The function of this gene is still unknown. Another 20 percent of familial cases result from mutations in the gene that encodes the enzyme copper-zinc superoxide dismutase 1 (SOD1).
Treatment:
No cure has yet been found for ALS. However, the Food and Drug Administration (FDA) approved the first drug treatment for the disease—riluzole (Rilutek)—in 1995. Riluzole is believed to reduce damage to motor neurons by decreasing the release of glutamate. Clinical trials with ALS patients showed that riluzole prolongs survival by several months, mainly in those with difficulty swallowing. The drug also extends the time before an individual needs ventilation support. Riluzole does not reverse the damage already done to motor neurons, and persons taking the drug must be monitored for liver damage and other possible side effects. However, this first disease-specific therapy offers hope that the progression of ALS may one day be slowed by new medications or combinations of drugs.
QUOTE FOR MONDAY:
A Japanese legend says that if you can’t sleep at night its because you are awake in someone else’s dream. (I must be in a lot of people’s dreams).
Insomnia
Insomnia is a sleeping disorder that is characterized by difficulty falling and/or staying asleep. People with Insomnia have one or more of the following symptoms:
- Difficulty falling asleep
- Waking up often during the night and having trouble going back to sleep
- Waking up too early in the morning
- Feeling tired upon waking * There are noted to be 2 types: Primary and Secondary
- Primary insomnia: Primary insomnia means that a person is having sleep problems that are not directly associated with any other health condition or problem.
- Secondary insomnia: Secondary insomnia means that a person is having sleep problems because of something else, such as a health condition (like asthma, depression, arthritis, cancer or heartburn). Other conditions could be pain, medication they are taking or a substance they are using (like alcohol). *AcuteInsomnia Insomnia also varies in how long it lasts and how often it occurs. It can be short-term (acute insomnia) or can last a long time (chronic insomnia). It can also come and go, with periods of time when a person has no sleep problems. Acute insomnia can last from one night to a few weeks. Insomnia is called chronic when a person has insomnia at least three nights a week for a month or longer.
- Significant life stress (job loss or change, death of a loved one, divorce, moving)
- Illness
- Emotional or physical discomfort
- Environmental factors like noise, light, or extreme temperatures (hot or cold) that interfere with sleep
- Some medications (for example those used to treat colds, allergies, depression, high blood pressure and asthma) which may interfere with sleep
- Interferences in normal sleep schedule ( jet lag or switching from a day to night shift, for example)
ChronicInsomnia caused by:
- Depression and/or anxiety
- Chronic stress
- Pain or discomfort at night
*Symptoms of insomnia can include:
- Sleepiness during the day
- General tiredness
- Irritability
- Problems with concentration or memory* How Insomnia can be diagnosed: If you think you have insomnia, talk to your health care provider or a doctor who majors in Insomnia. An evaluation may include a physical, a medical history, and a sleep history. You may be asked to keep a sleep diary for a week or two, keeping track of your sleep patterns and how you feel during the day. Your health care provider may want to interview your bed partner about the quantity and quality of your sleep. In some cases, you may be referred to a sleep center for special tests.* Treatment of InsomniaYou should seek help if your insomnia has become a pattern, or if you often feel fatigued or unrefreshed during the day and it interferes with your daily life. Many people have brief periods of difficulty sleeping (for example, a few days after starting a new job), but if insomnia lasts longer or has become a regular occurrence, you should ask for help.If you don’t feel satisfied after your conversation with your primary care physician, ask for a referral to a doctor who specializes in sleep medicine or consult other available resources. It’s important to find a doctor who has the proper knowledge and training to treat your insomnia.
- Non-Medical (Cognitive & Behavioral) Treatments for InsomniaSome of these techniques can be self-taught, while for others it’s better to enlist the help of a therapist or sleep specialist.
- Stimulus control helps to build an association between the bedroom and sleep by limiting the type of activities allowed in the bedroom. An example of stimulus control is going to bed only when you are sleepy, and getting out of bed if you’ve been awake for 20 minutes or more. This helps to break an unhealthy association between the bedroom and wakefulness. Sleep restriction involves a strict schedule of bedtimes and wake times and limits time in bed to only when a person is sleeping.
- Medical Treatments for InsomniaDetermining which medication may be right for you depends on your insomnia symptoms and many different health factors. This is why it’s important to consult with a doctor before taking a sleep aid.
- Alternative Medicine
- Major classes of prescription insomnia medications include benzodiazepine hypnotics, non-benzodiazepine hypnotics, and melatonin receptor agonists.
- There are many different types of sleep aids for insomnia, including over-the-counter (non-prescription) and prescription medications.
- Cognitive behavioral therapy (CBT) includes behavioral changes (such as keeping a regular bedtime and wake up time, getting out of bed after being awake for 20 minutes or so, and eliminating afternoon naps) but it adds a cognitive or “thinking” component. CBT works to challenge unhealthy beliefs and fears around sleep and teach rational, positive thinking. There is a good amount of research supporting the use of CBT for insomnia. For example, in one study, patients with insomnia attended one CBT session via the internet per week for 6 weeks. After the treatment, these people had improved sleep quality.
- Relaxation training, or progressive muscle relaxation, teaches the person to systematically tense and relax muscles in different areas of the body. This helps to calm the body and induce sleep. Other relaxation techniques that help many people sleep involve breathing exercises, mindfulness, meditation techniques, and guided imagery.
- Many people listen to audio recordings to guide them in learning these techniques. They can work to help you fall asleep and also return to sleep in the middle of the night.
- There are psychological and behavioral techniques that can be helpful for treating insomnia. Relaxation training, stimulus control, sleep restriction, and cognitive behavioral therapy are some examples.
- Many cities also have sleep centers and clinics (sometimes connected to a hospital) that offer assessments, testing, and treatment. An Internet search will help you locate the nearest center.
- Start by calling your primary care physician or bringing up the topic of sleep at your next well visit if you have one scheduled. If your doctor is knowledgeable about sleep disorders, he or she will guide you through the next steps, which may involve an assessment and further testing, or a referral to a sleep specialist. Your doctor may also start by giving you some basic information and resources about healthy sleep habits—these behavioral tips may help certain people with insomnia—or discussing potential medical treatment options to consider. Your doctor could refer you to a psychotherapist if your sleep struggles seem connected to anxiety, depression, or a major life adjustment. There are alternative medicines that may help certain people sleep. It’s important to know that these products are not required to pass through the same safety tests as medications, so their side effects and effectiveness are not as well understood.
QUOTE FOR THURSDAY:
“A Baker’s cyst, also called a popliteal (pop-luh-TEE-ul) cyst, is usually the result of a problem with your knee joint, such as arthritis or a cartilage tear.”
MAYO CLINIC
What is a Baker cyst?
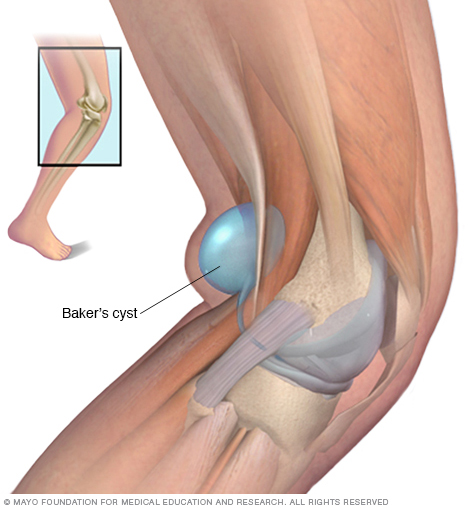
A Baker cyst is swelling caused by fluid from the knee joint protruding to the back of the knee. The back of the knee is also referred to as the popliteal area of the knee. A Baker cyst is sometimes referred to as a popliteal cyst. When an excess of knee joint fluid is compressed by the body weight between the bones of the knee joint, it can become trapped and separate from the joint to form the fluid-filled sac of a Baker cyst. The name of the cyst is in memory of the physician who originally described the condition, the British surgeon William Morrant Baker (1839-1896).
- A Baker cyst is swelling caused by fluid from the knee joint protruding to the back of the knee.
- Baker cysts are common and can be caused by virtually any cause of joint swelling (arthritis).
- A Baker cyst may not cause symptoms or be associated with knee pain and/or tightness behind the knee, especially when the knee is extended or fully flexed.
- Baker cysts can rupture and become complicated by spread of fluid down the leg between the muscles of the calf (dissection).
- Baker cysts can be treated with medications, joint aspiration and cortisone injection, and surgical operation, usually arthroscopic surgery.SIGNS & SYMPTOMS OF BAKER CYSTS:Baker cysts can become complicated by spread of fluid down the leg between the muscles of the calf (dissection). The cyst can rupture, leaking fluid down the inner leg to sometimes cause the appearance of a painless bruise under the inner ankle. Baker cyst dissection and rupture are frequently associated with swelling of the leg and can mimic phlebitis of the leg. A ruptured Baker cyst typically causes rapid-onset swelling of the leg.How is a Baker cyst treated? Baker cysts often resolve with aspiration (removal) of excess knee fluid in conjunction with cortisone injection. Medications are sometimes given to relieve pain and inflammation.
- DIAGNOSING BAKER CYSTS: Baker cysts can be diagnosed by the doctor’s examination and confirmed by imaging tests (either ultrasound, injection of contrast dye into the knee followed by imaging, called an arthrogram, or MRI scan) if necessary.
- A Baker cyst may cause no symptoms or be associated with knee pain and/or tightness behind the knee, especially when the knee is extended or fully flexed. Baker cysts are usually visible as a bulge behind the knee that is particularly noticeable on standing and when compared to the opposite uninvolved knee. They are generally soft and minimally tender.
- Baker cysts are not uncommon and can be caused by virtually any cause of joint swelling (arthritis). The excess joint fluid (synovial fluid) bulges to the back of the knee to form the Baker cyst. The most common type of arthritis associated with Baker cysts is osteoarthritis, also called degenerative arthritis. Baker cysts can occur in children with juvenile arthritis of the knee. Baker cysts also can result from cartilage tears (such as a torn meniscus), rheumatoid arthritis, and other knee problems.
When cartilage tears or other internal knee problems are associated, physical therapy or surgery can be the best treatment option. During a surgical operation, the surgeon can remove the swollen tissue (synovium) that leads to the cyst formation. This is most commonly done with arthroscopic surgery.
QUOTE FOR WEDNESDAY:
There is no disease more conducive to clinical humility than aneurysm of the aorta.
William Osler (July 12, 1849 – December 29, 1919 — was a Canadian physician and one of the four founding professors of Johns Hopkins Hospital.)
What is an aortic aneurysm?


The aorta is the large artery that exits in the heart and delivers blood to the body. It begins at the aortic valve that separates the left ventricle of the heart from the aorta and prevents blood from leaking back into the left ventricle after a contraction, which is actually when the heart pumps blood. The various sections of the aorta are named based upon “arch-like” initial design and the location of the aorta in the body. Thus, the beginning of the aorta is referred to as the ascending aorta (basically meaning the blood going against resistance due to the vessel being a hill for the blood to go up), followed by the arch of the aorta, then the descending aorta (which is the blood going downward via gravity with the help of the heart pumping the blood of course). The portion of the aorta that is located in the chest (called thorax) is referred to as the thoracic aorta, while the abdominal aorta (the part of the aorta below the thorax region) is located in the abdomen. The abdominal aorta extends from the diaphragm (at the bottom of the lungs like a floor to divide the lungs from the organs in the abdomen) to the mid-abdomen where it splits into the iliac arteries and when it reaches the legs the femoral arteries now start which supplies to the legs oxygenated blood. This is why commonly a cardiac catheterization to visualize the aorta and sometimes the left side of the heart is done starting in the femoral artery since in time it diverts into starting the abdominal aorta.
An aneurysm is an area of a localized widening (dilation) of a blood vessel. The word “aneurysm” is borrowed from the Greek “aneurysma” meaning “a widening”.
An aortic aneurysm involves the aorta, the major artery that leaves the heart to supply blood to the body. An aortic aneurysm is a dilation or bulging of the aorta..
Most aortic aneurysms are fusiform. They are shaped like a spindle (“fusus” means spindle in Latin) with widening all around the circumference of the aorta. (Saccular aneurysms just involve a portion of the aortic wall with a localized out pocketing).
What is inside an aortic aneurysm?
The inside walls of aneurysms are often lined with a blood clot that forms because there is stagnant blood. The wall of an aneurysm is layered, like a piece of plywood.
Who is most likely to have an abdominal aortic aneurysm?
Abdominal aortic aneurysms tend to occur in white males over the age of 60. In the United States, these aneurysms occur in up to 3.0% of the population. Aneurysms start to form at about age 50 and peak at age 80. Women are less likely to have aneurysms than men and African Americans are less likely to have aneurysms than Caucasians.
There is a genetic component that predisposes one to developing an aneurysm; the prevalence in someone who has a first-degree relative with the condition can be as high as 25%.
Collagen vascular diseases that can weaken the tissues of the aortic walls are also associated with aortic aneurysms. These diseases include Marfan syndrome and Ehlers-Danlos syndrome
Aortic aneurysms can develop anywhere along the length of the aorta but the majority are located in the abdominal aorta. Most of these abdominal aneurysms are located below the level of the renal arteries, the vessels that provide blood to the kidneys. Abdominal aortic aneurysms can extend into the iliac arteries.
What shape are most aortic aneurysms?
Most aortic aneurysms are fusiform. They are shaped like a spindle (“fusus” means spindle in Latin) with widening all around the circumference of the aorta. (Saccular aneurysms just involve a portion of the aortic wall with a localized out pocketing).
What is inside an aortic aneurysm?
The inside walls of aneurysms are often lined with a blood clot that forms because there is stagnant blood. The wall of an aneurysm is layered, like a piece of plywood.
Who is most likely to have an abdominal aortic aneurysm?
Abdominal aortic aneurysms tend to occur in white males over the age of 60. In the United States, these aneurysms occur in up to 3.0% of the population. Aneurysms start to form at about age 50 and peak at age 80. Women are less likely to have aneurysms than men and African Americans are less likely to have aneurysms than Caucasians.
There is a genetic component that predisposes one to developing an aneurysm; the prevalence in someone who has a first-degree relative with the condition can be as high as 25%.
Collagen vascular diseases that can weaken the tissues of the aortic walls are also associated with aortic aneurysms. These diseases include Marfan syndrome and Ehlers-Danlos syndrome.
What are risk factors for aortic aneurysms?
The risk factors for aortic aneurysm are the same as those for atherosclerotic heart disease, stroke, and peripheral artery disease and include:
- Cigarette smoking: This not only increases the risk of developing an abdominal aortic aneurysm, but also increases the risk of aneurysm rupture. Aortic rupture is a life-threatening event where blood escapes the aorta and the patient can quickly bleed to death.
- Elevated blood cholesterol levels
- Diabetes mellitus The most common cause of aortic aneurysms is “hardening of the arteries” called arteriosclerosis. At a majority of aortic aneurysms are from arteriosclerosis. The arteriosclerosis can weaken the aortic wall and the increased pressure of the blood being pumped through the aorta causes weakness of the inner layer of the aortic wall.Smoking is a major cause of aortic aneurysm. Studies have shown that the rate of aortic aneurysm has fallen at the same rate as population smoking rates.
- The aortic wall has three layers, the tunica adventitia, tunica media, and tunica intima. The layers add strength to the aorta as well as elasticity to tolerate changes in blood pressure. Chronically increased blood pressure causes the media layer to break down and leads to the continuous, slow dilation of the aorta.
- What is the most common cause of aortic aneurysms?