
Than when AV nodes which can be blocked=atrio-ventricular block (AV heart block)=HB is a type of heart block in which the conduction between the atria and ventricles of the heart is impaired. Under normal conditions, the sinoatrial node (SA node) in the atria sets the intial pace for the heart, and these impulses travel down to the atriums than passing the AV valves into the ventricles and up the purkinje fibers . In an AV block, this message does not reach the ventricles or is impaired along the way. The ventricles of the heart have their own pacing mechanisms, which can maintain a lowered heart rate in the absence of SA stimulation.
The causes of pathological AV block are varied and include ischemia, infarction, fibrosis or drugs, and the blocks may be complete or may only impair the signaling between the SA and AV nodes.
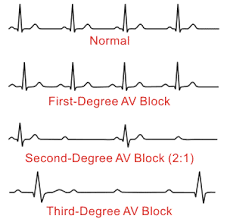
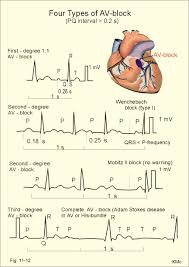
Types of AV blocks: 1st degree HB which is NSR with a prolonged PR interval and can live a totally normal life with it. PR interval is the time from beginning of the p wave to the beginning of the qrs wave. In all degrees of HB the PRI interval is prolonged. You can live a normal life with 1st degree HB.
Mobitz type I is benign, and most people do not experience symptoms. A doctor may only discover the condition during a routine exam or when checking for other conditions using an ECG. Those who do not experience symptoms may require monitoring on an outpatient basis. If people do experience symptoms, they may require treatment.
2nd degree HB-Mobitz I called Wenkebach is a NSR with a progressing increasing PR interval longer and longer till it actually drops a QRS and you see just the p wave without a QRS once and the rhythm restarts the pattern all over again.
Than 2nd degree HB-Mobitz II and this is a NSR with a prolonged PRI that measures the same amount each time but even though its not progressively getting longer its worse than Mobitz I always. This is because with the same measurement prolonged PRI interval you only see 2 or 3 more p waves without the QRS and these need immediate external subcutaneous pacing or just as effective if its not available (external subcutaneous pacing) than a dopamine IV drip 5-20 mcg/kg/min or epinephrine IV drip 2 to 10 mcg/min or epinephrine IV drip 2-10 mcg/min (not kg based).
Than there is complete HB 3rd degree heart block where no conduction from atriums to ventricles is going through so the atriums are contracting the way they want and the ventricles contracting the way they want. The problem is there is a total disassociation between the upper and lower chambers. Treatment for most patients with acquired complete heart block will require a permanent pacemaker or an implantable cardioverter defibrillator (ICD). Temporarily till OR the pt may have subcutaneous pacing but may not work at in some cases.