Arthritis is a joint disease ((Medically Arthro means joint / itis means inflammation). The main symptoms of arthritis are joint pain and stiffness, which typically worsen with age. A joint exists where the ends of two or more bones meet. The knee joint, for example, is formed between the bones of the lower leg (tibia and fibula) and the thighbone (femur). The hip joint is located where the top of the thighbone (femoral head) meets the cup portion of the pelvis (acetabulum).
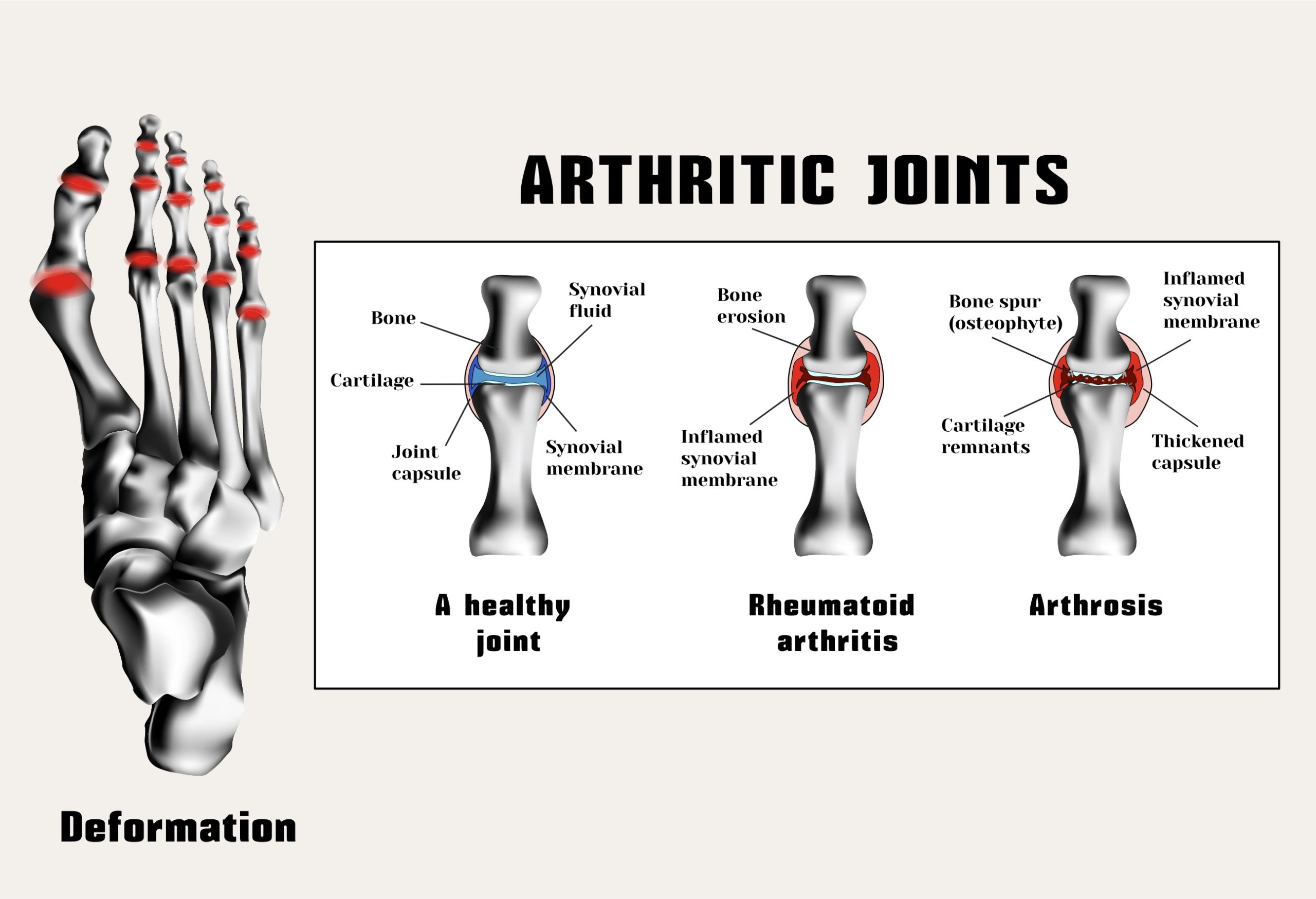
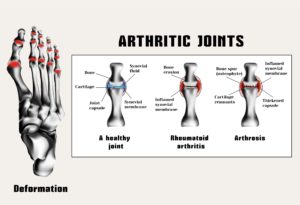
Cartilage. A smooth layer of cartilage covers the ends of bones in a joint. Cartilage cushions the bone and allows the joint to move easily without the friction that would occur with bone-on-bone contact.
Synovium. A joint is enclosed by a fibrous capsule that is lined with a tissue called the synovium, which produces a fluid that also helps to reduce friction and wear in a joint.
Muscles, tendons, and ligaments. Ligaments connect the bones and keep the joint stable. Muscles and tendons power the joint and enable it to move.
Osteoarthritis causes cartilage — the hard, slippery tissue that covers the ends of bones where they form a joint — to break down. Rheumatoid arthritis is a disease in which the immune system attacks the joints, beginning with the lining of joints.
Uric acid crystals, which form when there’s too much uric acid in your blood, can cause gout. Infections or underlying disease, such as psoriasis or lupus, can cause other types of arthritis.
Treatments vary depending on many factors but first the type of arthritis. The main goals of arthritis treatments are to reduce symptoms and improve quality of life.
Types of Arthritis:
1-Rheumatoid Arthritis (RA) symptoms are joint inflammation that comes from pain, warmth, and swelling. The inflammation is typically symmetrical that is occurring on both sides of the body at the same time (such as hands, wrists, or knees). Other signs of Rheumatoid Arthritis include joint stiffness that is particularly in the AM upon awakening or after periods of inactivity; ongoing fatigue, and low-grade fever. Signs and symptoms come about gradually over years but can come on rapidly for some other people. RA is while is an autoimmune disorder.
2-Osteoarthritis is usually caused by normal wear and tear, while rheumatoid arthritis is an autoimmune disorder. Other types of arthritis can be caused by uric acid crystals, infections or even an underlying disease, such as psoriasis or lupus.
3-Autoimmune Inflammatory Arthritis
A healthy immune system is protective. It generates inflammation to clear infections and heal injuries. But in inflammatory arthritis, the immune system is overactive, attacking healthy tissue, including joints in the spine, hands and feet. In some people, inflammation becomes systemic, damaging the eyes, skin, heart and other organs. Many, but not all types of inflammatory arthritis are considered autoimmune diseases because the immune system loses the ability to distinguish self from not-self and attacks the body it’s supposed to protect.
Rheumatoid arthritis (RA) is the most common form of autoimmune inflammatory arthritis. Psoriatic arthritis (PsA) axial spondyloarthritis (axSpA), gout and juvenile arthritis are less common and can be more challenging to diagnose.
4-Infectious Arthritis
A bacterial, viral or fungal infection triggers infectious arthritis. It usually starts when an infection from another part of the body travels to a joint, usually the knee. Symptoms like swelling, pain and fever can be sudden and intense, but treatment with antibiotics or antifungals usually clears the infection pretty quickly. Most viral infections last a week or two and go away on their own. Some people with infectious arthritis may need to have their joint fluid drained to remove infected synovial fluid, reduce pain and inflammation and prevent joint damage.
5-Gout (Metabolic Arthritis)
Metabolic or gouty arthritis — commonly known as gout — results from a buildup in joints of painful uric acid crystals. These are a byproduct of the breakdown of purines — substances normally found in human cells and many foods, especially red meat, organ meats, some seafoods and alcohol. Normally the body gets rid of excess uric acid, but when it doesn’t, it can accumulate in joints, causing sudden and intense bouts of pain, especially the big toe.
However, most people with high uric acid levels never develop gout and many gout patients have normal uric acid. Some research suggests that certain factors in addition to uric acid might trigger gout. Possible culprits include damage from OA, disruptions in the microbiome and even white blood cells in the fluid inside joints.
Some people experience only one gout attack, or flare, and never have other symptoms. They don’t typically require medication. People who have more than one gout flare or severe symptoms are typically prescribed uric acid-lowering drugs. Those drugs can have serious side effects (and may not address the real problem), so in addition to taking medication, patients are advised to adopt a mostly plant-based, low-purine diet, rich in fruit, vegetables, whole grains, olive oil and low-purine fish.
6-Ankylosing spondylitis is a type of arthritis that causes inflammation in the joints and ligaments of the spine.
Regardless of whether arthritis is caused by injury, normal wear and tear, or systemic disease, the affected joint becomes inflamed, causing swelling, pain, and stiffness. Inflammation is one of the body’s normal reactions to injury or disease. In arthritic joints, however, inflammation may cause long-lasting or permanent disability when it destroys the joint’s cartilge.
The most common types of arthritis are osteoarthritis and rheumatoid arthritis.
The most common signs and symptoms of arthritis involve the joints:
- Pain
- Stiffness
- Swelling
- Redness
- Decreased range of motion
How arthritis is diagnosed:
Laboratory tests
The analysis of different types of body fluids can help pinpoint the type of arthritis you may have. Fluids commonly analyzed include blood, urine and joint fluid. To obtain a sample of joint fluid, doctors cleanse and numb the area before inserting a needle in the joint space to withdraw some fluid.
Imaging
These types of tests can detect problems within the joint that may be causing your symptoms. Examples include:
- X-rays. Using low levels of radiation to visualize bone, X-rays can show cartilage loss, bone damage and bone spurs. X-rays may not reveal early arthritic damage, but they are often used to track progression of the disease.
- Computerized tomography (CT). CT scanners take X-rays from many different angles and combine the information to create cross-sectional views of internal structures. CTs can visualize both bone and the surrounding soft tissues.
- Magnetic resonance imaging (MRI). Combining radio waves with a strong magnetic field, MRIs can produce more-detailed cross-sectional images of soft tissues such as cartilage, tendons and ligaments.
- Ultrasound. This technology uses high-frequency sound waves to image soft tissues, cartilage and fluid-containing structures near the joints (bursae). Ultrasound is also used to guide needle placement for removing joint fluid or injecting medications into the joint.
Treatments for arthritis:
Arthritis treatment focuses on relieving symptoms and improving joint function. You may need to try several different treatments, or combinations of treatments, before you determine what works best for you.
Medications
The medications used to treat arthritis vary depending on the type of arthritis. Commonly used arthritis medications include:
- NSAIDs. Nonsteroidal anti-inflammatory drugs (NSAIDs) can relieve pain and reduce inflammation. Examples include ibuprofen (Advil, Motrin IB, others) and naproxen sodium (Aleve). Stronger NSAIDs can cause stomach irritation and may increase your risk of heart attack or stroke. NSAIDs are also available as creams or gels, which can be rubbed on joints.
- Counterirritants. Some varieties of creams and ointments contain menthol or capsaicin, the ingredient that makes hot peppers spicy. Rubbing these preparations on the skin over your aching joint may interfere with the transmission of pain signals from the joint itself.
- Steroids. Corticosteroid medications, such as prednisone, reduce inflammation and pain and slow joint damage. Corticosteroids may be given as a pill or as an injection into the painful joint. Side effects may include thinning of bones, weight gain and diabetes.
- Disease-modifying antirheumatic drugs (DMARDs). These drugs can slow the progression of rheumatoid arthritis and save the joints and other tissues from permanent damage. In addition to conventional DMARDs, there are also biologic agents and targeted synthetic DMARDs. Side effects vary but most DMARDs increase your risk of infections.
Therapy
Physical therapy can be helpful for some types of arthritis. Exercises can improve range of motion and strengthen the muscles surrounding joints. In some cases, splints or braces may be warranted.
Surgery
If conservative measures don’t help, doctors may suggest surgery, such as:
- Joint repair. In some instances, joint surfaces can be smoothed or realigned to reduce pain and improve function. These types of procedures can often be performed arthroscopically — through small incisions over the joint.
- Joint replacement. This procedure removes the damaged joint and replaces it with an artificial one. Joints most commonly replaced are hips and knees.
- Joint fusion. This procedure is more often used for smaller joints, such as those in the wrist, ankle and fingers. It removes the ends of the two bones in the joint and then locks those ends together until they heal into one rigid unit.