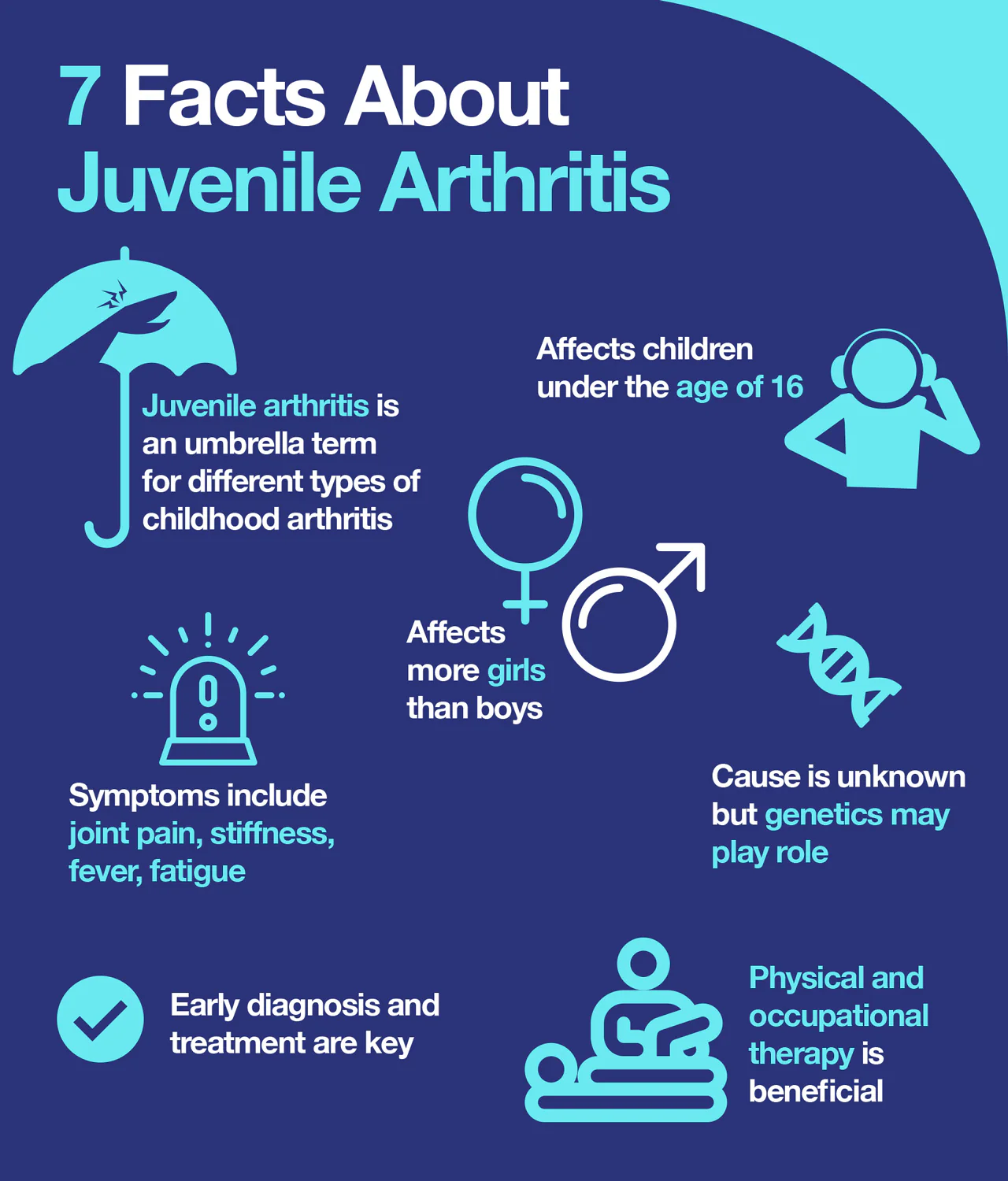
“Juvenile idiopathic arthritis, formerly known as juvenile rheumatoid arthritis, is the most common type of arthritis in children under the age of 16.
Juvenile idiopathic arthritis occurs when the body’s immune system attacks its own cells and tissues. It’s not known why this happens, but both heredity and environment seem to play a role. Some forms of juvenile idiopathic arthritis are more common in girls.”
MAYO CLINIC (https://www.mayoclinic.org/diseases-conditions/juvenile-idiopathic-arthritis/symptoms-causes/syc-20374082)”
Diagnosis of juvenile idiopathic arthritis can be difficult because joint pain can be caused by many different types of problems. No single test can confirm a diagnosis, but tests can help rule out some other conditions that produce similar signs and symptoms.
1. Blood tests
Some of the most common blood tests for suspected cases include:
Erythrocyte sedimentation rate (ESR). The sedimentation rate is the speed at which your red blood cells settle to the bottom of a tube of blood. An elevated rate can indicate inflammation. Measuring the ESR is primarily used to determine the degree of inflammation.
C-reactive protein. This blood test also measures levels of general inflammation in the body but on a different scale than the ESR.
Antinuclear antibody. Antinuclear antibodies are proteins commonly produced by the immune systems of people with certain autoimmune diseases, including arthritis. They are a marker for an increased chance of eye inflammation.
Rheumatoid factor. This antibody is occasionally found in the blood of children who have juvenile idiopathic arthritis and may mean there’s a higher risk of damage from arthritis.
Cyclic citrullinated peptide (CCP). Like the rheumatoid factor, the CCP is another antibody that may be found in the blood of children with juvenile idiopathic arthritis and may indicate a higher risk of damage.
In many children with juvenile idiopathic arthritis, no significant abnormality will be found in these blood tests.
2. Imaging scans
X-rays or magnetic resonance imaging may be taken to exclude other conditions, such as fractures, tumors, infection or congenital defects.
Imaging may also be used from time to time after the diagnosis to monitor bone development and to detect joint damage.
Juvenile Arthritis (JIA) Treatment:
Treatment for juvenile idiopathic arthritis focuses on helping your child maintain a normal level of physical and social activity. To accomplish this, doctors may use a combination of strategies to relieve pain and swelling, maintain full movement and strength, and prevent complications.
1. Medications
The medications used to help children with juvenile idiopathic arthritis are chosen to decrease pain, improve function and minimize potential joint damage.
Typical medications include:
Nonsteroidal anti-inflammatory drugs (NSAIDs). These medications, such as ibuprofen (Advil, Motrin, others) and naproxen sodium (Aleve), reduce pain and swelling. Side effects include stomach upset and, much less often, kidney and liver problems.
Disease-modifying antirheumatic drugs (DMARDs). Doctors use these medications when NSAIDs alone fail to relieve symptoms of joint pain and swelling or if there is a high risk of damage in the future.DMARDs may be taken in combination with NSAIDs and are used to slow the progress of juvenile idiopathic arthritis. The most commonly used DMARD for children is methotrexate (Trexall, Xatmep, others). Side effects of methotrexate may include nausea, low blood counts, liver problems and a mild increased risk of infection.
Biologic agents. Also known as biologic response modifiers, this newer class of drugs includes tumor necrosis factor (TNF) blockers, such as etanercept (Enbrel, Erelzi, Eticovo), adalimumab (Humira), golimumab (Simponi) and infliximab (Remicade, Inflectra, others). These medications can help reduce systemic inflammation and prevent joint damage. They may be used with DMARDs and other medications.Other biologic agents work to suppress the immune system in slightly different ways, including abatacept (Orencia), rituximab (Rituxan, Truxima, Ruxience), anakinra (Kineret) and tocilizumab (Actemra). All biologics can increase the risk of infection.
Corticosteroids. Medications such as prednisone may be used to control symptoms until another medication takes effect. They are also used to treat inflammation when it is not in the joints, such as inflammation of the sac around the heart.These drugs can interfere with normal growth and increase susceptibility to infection, so they generally should be used for the shortest possible duration.
2. Therapies
Your doctor may recommend that your child work with a physical therapist to help keep joints flexible and maintain range of motion and muscle tone.
A physical therapist or an occupational therapist may make additional recommendations regarding the best exercise and protective equipment for your child.
A physical or occupational therapist may also recommend that your child make use of joint supports or splints to help protect joints and keep them in a good functional position.
3. Surgery
In very severe cases, surgery may be needed to improve joint function.
***Parents or caregivers help limit the arthritis in your children by doing the following:
Getting regular exercise. Exercise is important because it promotes both muscle strength and joint flexibility. Swimming is an excellent choice because it places minimal stress on joints.
Applying cold or heat. Stiffness affects many children with juvenile idiopathic arthritis, particularly in the morning. Some children respond well to cold packs, particularly after activity. However, most children prefer warmth, such as a hot pack or a hot bath or shower, especially in the morning
Eating Well. Some children with arthritis have poor appetites. Others may gain excess weight due to medications or physical inactivity. A healthy diet can help maintain an appropriate body weight.Know adequate calcium in the diet is important because children with juvenile idiopathic arthritis are at risk of developing weak bones due to the disease, the use of corticosteroids, and decreased physical activity and weight bearing.
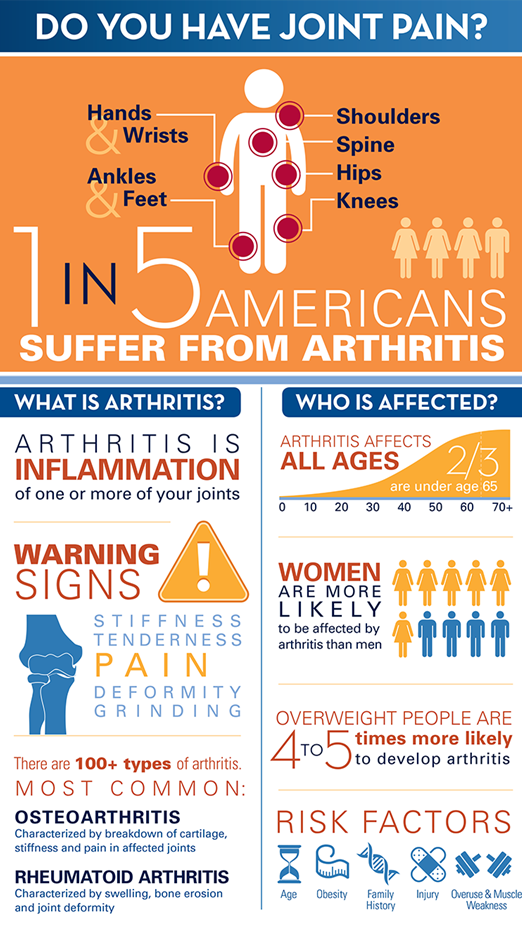
“Arthritis affects persons of all ages; little is known about arthritis prevalence among children and adolescents aged <18 years.
Approximately 220,000 children and adolescents had arthritis during 2017–2021. Prevalence increased with age and was highest among those aged 12–17 years, non-Hispanic Black or African American children and adolescents, children and adolescents with anxiety or depression, those who were physically inactive, had overweight or a heart condition, or lived in a food-insecure or smoking household.
Arthritis affects persons of all ages, including younger adults, adolescents, and children; however, recent arthritis prevalence estimates among children and adolescents aged <18 years are not available. Previous prevalence estimates among U.S. children and adolescents aged <18 years ranged from 21 to 403 per 100,000 population depending upon the case definition used. CDC analyzed aggregated 2017–2021 National Survey of Children’s Health data to estimate the national prevalence of parent-reported arthritis diagnosed among children and adolescents aged <18 years. An estimated 220,000 (95% CI = 187,000–260,000) U.S. children and adolescents aged <18 years (305 per 100,000) had diagnosed arthritis. Arthritis prevalence among non-Hispanic Black or African American children and adolescents was twice that of non-Hispanic White children and adolescents.”
What is Juvenile Arthritis (JIA) and how different is it than adults with a type of arthritis?
Like adults, children can develop arthritis. The most common type of chronic, or long-lasting, arthritis that affects children is called juvenile idiopathic arthritis (JIA). JIA broadly refers to several different chronic disorders involving inflammation of joints (arthritis), which can cause joint pain, swelling, warmth, stiffness, and loss of motion. The various forms of JIA have different features, such as the pattern of joints involved and inflammation of other parts of the body besides the joints. JIA may last a limited time, such as a few months or years, but in some cases it is a lifelong disease that requires treatment into adulthood.
JIA is “idiopathic,” meaning that its origins are not understood. While the exact causes of JIA are unknown, it begins when the immune system becomes overactive and creates inflammation.
With treatment, most children achieve periods of wellness (remission), and sometimes the disease goes away permanently with no further need for medications. It is important to see a doctor early if your child has swollen or stiff joints because delaying therapy can lead to joint damage, a lesser response to treatment, and other problems.
Who Gets Juvenile Idiopathic Arthritis (JIA)?
By definition, JIA begins in children and adolescents before the 16th birthday. Most types of the disease are more frequent in girls, but enthesitis-related JIA, a form of the disease that involves inflammation of the places where ligaments and tendons (flexible bands of tissue) attach to bones, is more common in boys. Systemic JIA, a rare type of JIA that features fever and rash, affects boys and girls equally. Children of all races and ethnic backgrounds can get the disease.
It is very rare for more than one member of a family to have JIA, but children with a family member with chronic arthritis, including JIA, are at a slightly increased risk of developing it. Having a family member with psoriasis is a risk factor for a form of JIA called psoriatic JIA.
There are many types of Juvenile Arthritis (JIA)with distinct features:
Generally, they all share arthritic symptoms of joint pain, swelling, warmth, and stiffness that last at least 6 weeks.
The types of JIA:
Oligoarticular juvenile idiopathic arthritis. This is the most common and mildest form, affecting four or fewer joints. It is considered persistent if symptoms continue for 6 months or longer, and extended if five or more joints become involved after 6 months of illness. Commonly affected joints are knees or ankles. A form of eye inflammation called chronic (long-lasting) uveitis can develop in children with this form of JIA. About half of children with JIA have this type.
Polyarticular juvenile idiopathic arthritis–rheumatoid factor negative. This is the second most common type, affecting five or more joints in the first 6 months. Tests for rheumatoid factor are negative. The rheumatoid factor blood test checks for autoimmune disease, especially rheumatoid arthritis, which is an adult form of arthritis. Some of these children develop chronic uveitis.
Polyarticular juvenile idiopathic arthritis–rheumatoid factor positive. A child with this type has arthritis in five or more joints during the first 6 months of the disease. Tests for rheumatoid factor, a marker for autoimmune disease, are positive. It tends to occur in preteen and teenage girls, and it appears to be essentially the same as adult rheumatoid arthritis.
Enthesitis-related juvenile idiopathic arthritis. This form of JIA involves both arthritis and enthesitis. Enthesitis happens when inflammation occurs where a ligament or tendon attaches to a bone. The most common locations for enthesitis are the knees, heels, and bottoms of the feet. Arthritis is usually in the hips, knees, ankles, and feet, but the sacroiliac joints (at the base of the back) and spinal joints can also become inflamed. Some children get episodes of acute anterior uveitis, a sudden onset of inflammation of the front of the eye. Unlike most other forms of JIA, enthesitis-related JIA is more common in boys.
Psoriatic juvenile idiopathic arthritis. Children with this type have psoriasis, a skin condition, as well as inflammation of the joints. The skin condition usually appears first, but sometimes painful, stiff joints are the first sign, with the skin disease occurring years layer. Pitted fingernails and dactylitis (swollen fingers or toes) are also signs of the disease.
Systemic juvenile idiopathic arthritis. Systemic means the disease can affect the whole body, not just a specific organ or joint. Systemic JIA usually starts with fever and rash that come and go over the span of at least 2 weeks. In many cases, the joints become inflamed, but sometimes not until long after the fever goes away, and sometimes not at all if treatment is started quickly. In severe forms, inflammation can develop in and around organs, such as the spleen, lymph nodes, liver, and linings of the heart and lungs. Systemic JIA affects boys and girls with equal frequency.
Undifferentiated arthritis. This category includes children who have symptoms that do not fit into any of the other types or that fit into more than one type.
If left untreated, uveitis can lead to eye problems such as cataracts, glaucoma, and vision loss, so it is important for children with JIA to have frequent eye exams.
Skin changes. Depending on the type of JIA a child has, he or she may develop skin changes. Children with:
Systemic JIA who have fevers can get a light red or pink rash that comes and goes.
Psoriatic JIA can develop scaly red patches of skin. Psoriatic JIA can also cause pitted nails and dactylitis (swollen fingers or toes).
Polyarticular JIA with rheumatoid factor can get small bumps or nodules on parts of the body that receive pressure, such as from sitting.
Fever. Patients with systemic JIA typically have daily fevers when the disease begins or flares. The fever usually appears in the evening, and the rash may move from one part of the body to another, usually happening with the fever. Patients with other types of JIA do not generally develop fevers.
Growth problems. Inflammation in children with any type of JIA can lead to growth problems. Depending on the severity of the disease and the joints involved, bones near inflamed joints may grow too quickly or too slowly. This can cause one leg or arm to be longer than the other, or can result in a small or misshapen chin. Overall growth also may be slowed if the disease is severe. Growth normally improves when inflammation is well-controlled through treatment.
Tune in tomorrow on the causes, how its diagnosed and treated!
While 4th of July is a time for barbecues and parties, it can also increase the risk for accidents and injuries. A recent survey found that unsafe fireworks displays and drunk driving are two of the biggest concerns for the upcoming holiday. Planning ahead – and prioritizing safety – are the keys to a safe and fun holiday. Fourth of July is right around the corner, and there’s no better time to start preparing for barbecues, trips, and celebrations.
The survey findings highlighted some of the biggest safety risks that pop up around this time of year:
Nearly 60% of respondents said they’ve seen unsafe fireworks use during 4th of July
About 33% of Gen Z and Millennial respondents said they’ve been pressured into risky behavior
Nearly 70% of respondents said they’ve seen someone try to drive drunk on 4th of July
Under 30% of respondents said they trust other Americans to celebrate responsibly
“Stick with people and activities you are familiar with,” Steadman said. “Don’t take unnecessary risks or get caught up in a crowd of unruly people. Be cognizant of children and others who may need extra looking after.
“The 4th of July is a time for celebration of America and freedom. By taking the necessary precautions and avoiding risky behavior, everyone can enjoy the day. Stay vigilant and be prepared for if things go south, and always make sure you are practicing safe behavior with both fireworks and alcohol.”
The Fourth of July is a time to celebrate with friends and family the vast opportunities our country has given us. While we reach the end of the COVID-19 pandemic, many Independence Day traditions and celebrations are a go, but that may not be the case everywhere. Be sure to check your local restrictions before hosting barbeques. If your state is fully opened and you plan to attend an event, be vigilant about your safety and that of your belongings. Here are a few other tips to help you get through the festivities.
WAYS TO STAY SAFE ON THE FOURTH OF JULY
Stay cool and hydrated especially in areas very hot!
July is one of the hottest times of the year and it’s easy to fall victim to sun or heat stroke. Stay cool by being a shade-seeker: bringing an umbrella with you, wearing a hat, or staying under the covered portion of a porch or patio. It’s equally as important to wear sunscreen as well as light and loose clothing.
Finally, don’t forget the water. Many times, we get caught up in festive food and drink options and forget to add in water. Aim for eight cups or more per day, depending on how hot it is outside or how much sweet or salty food you are consuming.
Consider the safety of your food
The heat not only has an impact on you but your food as well. Having a BBQ and thinking of throwing all the meat on one platter outside awaiting the grill? Think again. Keep raw meat and seafood cold until it’s ready to be cooked. Once it’s ready, keep it hot until it’s consumed, then put in the fridge once everyone is done, meaning, don’t let it sit out. Contaminated food or items that have sat out too long can lead to food poisoning of some sickness, like infection.
Be mindful at events
Summer and celebrations mean concerts, BBQs, and state or county fairs. But it’s important to always be aware of your surroundings. Don’t leave your food, bag, or belongings unattended, and if the event is happening at night, be sure to stick with a friend. Fireworks are prime for theft as they are loud with those watching focused on the show.
4. Prevent eye injury
Prevent Blindness Texas has declared June 28th through July 4th as Fireworks Safety Awareness Week. Fireworks can damage your eyes, too. Contusions and lacerations are the most frequent injuries to eyes, which include foreign bodies in the eye.
If you do encounter an eye emergency, follow these steps to save your sight.
In the event of an eye emergency:
Do not rub the eye. Rubbing the eye may increase bleeding or make the injury worse.
Do not attempt to rinse out the eye. This can be even more damaging than rubbing.
Do not apply pressure to the eye itself. Holding or taping a foam cup or the bottom of a juice carton to the eye are just two tips. Protecting the eye from further contact with any item, including your hand, is the goal.
Do not stop for medicine! Over-the-counter pain relievers will not do much to relieve pain. Aspirin (should never be given to children) and Ibuprofen can thin the blood and increase bleeding. Go to the emergency room at once – this is more important than stopping for a pain reliever.
Do not apply ointment. Ointment, which may not be sterile, makes the area around the eye slippery and harder for the doctor to examine.
Overall, the best way to prevent eye or other injuries is to not play with fireworks and do not let your child play with fireworks, even if their friends are.
“If your holiday plans include fun in the water, make sure every member of your family is water smart ─ has swimming skills and knows how to help others in an emergency.
The American Red Cross offers these tips to help keep you and your loved ones safe during the upcoming 4th of July holidaay:
FIREWORKS SAFETY The safest way to enjoy fireworks is to attend a public fireworks show put on by professionals. Many states outlaw most fireworks, so consider celebrating with glow sticks, noise makers or silly string instead. If you choose to set fireworks off at home, follow these safety steps:
Never give fireworks to small children, and never throw or point a firework toward people, animals, vehicles, structures or flammable materials.
Always follow the instructions on the packaging.
Keep a supply of water close by.
Make sure the person lighting fireworks always wears eye protection.
Light only one firework at a time and never attempt to relight “a dud.”
Store fireworks in a cool, dry place away from children and pets.
Never use fireworks around pets, keep pets indoors. Exposure to lit fireworks can potentially result in severe burns or trauma, and many pets are also fearful of loud noises and can become lost, scared or disoriented.
WATER SAFETY If your holiday plans include fun in the water, make sure every member of your family is water smart ─ has swimming skills and knows how to help others in an emergency.
Everyone should learn to swim. Classes are available for both children and adults.
Prevent unsupervised access to water. Always designate a “water watcher” to keep a close, constant eye on everyone in and around the water until the next water watcher takes over.
Avoid distractions when supervising children. If a child is missing, check the water first. Drowning behavior is typically fast and silent. Unless rescued, a drowning person will last only 20 to 60 seconds before submerging.
Reach or throw, don’t go! In the event of an emergency, reach or throw an object out to the person in trouble and tell them to grab on. Don’t go in! You could become a victim yourself. Without putting yourself in danger, rescue and remove the person from the water. Have someone call 911 if needed.”
Were saying to celebrate the 4th of July but what we are saying is be SAFE, SAFE, SAFE!
The Fourth of July is a time for America to commemorate the passage of the Declaration of Independence and often celebrated with parades, concerts, firework shows, family road trips, barbeques, and parties where participants toast to the nation.
Sadly, these holiday festivities can lead to potentially deadly consequences on the roads, especially when alcohol is thrown into the mix. According to the National Highway Traffic and Safety Administration, 812 people died in motor vehicle crashes involving drunk drivers during the July 4th holiday period from 2014-2018.
“Many of our service members and their families will take to the roads in hopes of celebrating our nation’s birthday someplace special,” said Michael Ballard, chief of occupational safety, Air Force Safety Center. “I urge leadership at all levels to take time to engage with Airmen and Guardians about having a plan to reduce the risks associated with their holiday weekend activities.”
On average, 10,200 home fires are started by a grill each year, with gas grills contributing to a higher number of fires than charcoal grills, according to the National Fire Protection Association.
The USFA reported that almost half (49%) of grill fires on residential properties occur between 5 and 8 p.m., with more than half (57%) occurring between May and August.
Nearly a third (32%) of grill fires on residential properties start on patios, terraces, screened-in porches or courtyards, while an additional 24% start on exterior balconies and unenclosed porches.
The leading power source of grill fires is “gas fuels,” with fires primarily being fueled by propane, according to the USFA.
The leading factors contributing to the ignition of these fires are mechanical failures or malfunctions, misuse of materials and operational deficiencies.
The Office of the Illinois State Fire Marshal advises everyone to take the following steps to help ensure safe grilling:
Propane and charcoal grills should be used only outdoors.
The grill should be placed away from the home or deck railing, and out from under the eaves of your home and overhanging tree branches.
Keep children and pets at least three feet away from the grilling area.
Keep your grill clean by removing grease or fat buildup from the grills and in the trays below the grill.
Never leave your grill unattended.
Always make sure gas grill lids are open before lighting it.
Check the gas tank on your propane grills and hoses for leaks each time before using.
If you smell gas while grilling, immediately get away from the grill and call the fire department.
Make sure charcoal grill coals are cool before disposing of them in a metal container.
Always have a fire extinguisher, bucket of water or garden hose nearby or know where you can access one quickly.
Campfires need to be built at least 25 feet way from tents, shrubs and anything that can burn. Make sure fires are allowed in the area where you are camping.
Use of chimneys, outdoor fireplaces and fire pits need to be at least 10 feet away from your home or anything that can burn.
You can find an easy-to-follow grill safety guide published by the USFA here.
According to the Insurance Institute for Highway Safety (IIHS), July 4th is historically the deadliest day of the year for traffic fatalities in the United States. This is primarily due to a combination of increased travel and alcohol consumption. The National Safety Council (NSC) projects that in 2025 alone, as many as 599 people could die in motor vehicle crashes during the holiday weekend.
What makes this time so hazardous? For one, over 43 million Americans are expected to travel during the holiday period, the majority of them by car. Heavy traffic, long travel times, and drivers unfamiliar with their routes create an environment ripe for accidents. Add alcohol into the mix, and the risks escalate dramatically.
In fact, over 40% of July 4th crash fatalities involve alcohol impairment. Drivers aged 21 to 34 are the highest risk group, who account for nearly half of all alcohol-related crash deaths during this period.
How to stay safe on the road:
Always wear your seatbelt. Seat belts reduce fatal injury risk by 45%.
Don’t drive under the influence of alcohol or drugs.
Plan your route ahead of time to avoid getting lost or fatigued.
Avoid driving late at night when impaired drivers are more likely to be on the road.
If you’re going out drinking, use a designated driver, rideshare app, or public transportation.
Never use your phone while driving.
Come on back for part II tomorrow on continuing with facts and safety tips!
“Question Does acetaminophen use during pregnancy increase children’s risk of neurodevelopmental disorders?
Findings In this population-based study, models without sibling controls identified marginally increased risks of autism and attention-deficit/hyperactivity disorder (ADHD) associated with acetaminophen use during pregnancy. However, analyses of matched full sibling pairs found no evidence of increased risk of autism (hazard ratio, 0.98), ADHD (hazard ratio, 0.98), or intellectual disability (hazard ratio, 1.01) associated with acetaminophen use.
Meaning Acetaminophen use during pregnancy was not associated with children’s risk of autism, ADHD, or intellectual disability in sibling control analyses. This suggests that associations observed in other models may have been attributable to confounding.”
Is Tylenol Linked to Autism? As early as 2008, researchers discovered a potential link between Tylenol and postnatal autism, and noted a rise in autism since 1980. During that period, the U.S. Centers for Disease Control and Prevention recommended substituting aspirin instead of acetaminophen for infants.
“Readers have asked whether Tylenol (acetaminophen) is connected to autism or ADHD, also known as attention-deficit/hyperactivity disorder. One person forwarded a sponsored Facebook post from the page “Child Autism & ADHD from Tylenol during pregnancy” stating that “parents of children with autism or ADHD whose mother took Tylenol while pregnant may be eligible for legal compensation.” The page continues to run similar advertisements, as do various other pages. Parents have filed lawsuits against retailers of acetaminophen, stating that their children developed autism or ADHD due to exposure to acetaminophen taken during pregnancy.
Some studies have indeed shown a relationship between acetaminophen taken during pregnancy and autism or ADHD in children, but they do not demonstrate that the acetaminophen use caused the elevated rates of autism and ADHD, researchers say. For example, a pregnant person who takes acetaminophen may have a child with ADHD or autism because of other factors, such as genetics.
Experts agree that acetaminophen has a role in pregnancy but that it should be used only when necessary and in consultation with a doctor. Avoiding use of acetaminophen for fever or pain during pregnancy may have negative consequences. For instance, an uncontrolled fever in early pregnancy can harm brain development.
A Food and Drug Administration spokesperson told us via email that the available evidence is “too limited to make any recommendations based on these studies at this time.”
The American College of Obstetricians and Gynecologists said in a 2021 statement that studies “show no clear evidence that proves a direct relationship between the prudent use of acetaminophen during any trimester and fetal developmental issues.” An ACOG representative told us that the statement is the most up-to-date communication on the topic. And a 2017 Society for Maternal-Fetal Medicine statement, which a representative also confirmed to be the most up-to-date document, found the evidence on a causal link between acetaminophen and neurobehavioral disorders to be “inconclusive.”
Studies of Acetaminophen During Pregnancy Have Weaknesses
Acetaminophen, called paracetamol outside the U.S., is used widely during pregnancy to treat pain and fever. It is an ingredient in many over-the-counter and prescription medications, including Tylenol, Excedrin and Vicodin, as well as some versions of DayQuil, NyQuil, Sudafed, Mucinex and Midol.
As we said, some studies have found that women who reported using acetaminophen during pregnancy were more likely than those who didn’t to have children who later developed autism or ADHD. A 2018 paper published in the American Journal of Epidemiology that aimed to comprehensively analyze data from multiple studies, for example, found a 34% and 19% higher risk of ADHD and autism, respectively, in children whose mothers took acetaminophen in pregnancy compared with those whose mothers did not.
But this doesn’t necessarily mean acetaminophen is to blame for the conditions.
These studies were observational, meaning that researchers simply noted levels of acetaminophen exposure, generally based on reports from the parents in the studies. Randomized controlled trials — in which one group receives a medication or treatment and another group receives a placebo or standard care — are the gold standard for determining whether a causal relationship exists.
It is possible that people who take more acetaminophen are more likely to have characteristics that predispose them to have a child with autism or ADHD — including the illnesses or other health conditions that might have prompted a pregnant person to take acetaminophen in the first place.
The authors of the 2018 study recognized this issue, writing that the results “should be interpreted with caution given that the available evidence consists of observational studies and is susceptible to several potential sources of bias.”
Sura Alwan, a birth defects epidemiologist and co-director of the Teratogen Information System at the University of Washington, told us in an email that genetic factors might also help explain the results, adding that not all studies have found an association between prenatal acetaminophen and neurodevelopmental outcomes like autism and ADHD.
In any case, she said, the studies “do not necessarily imply a causal link, which means that there isn’t enough evidence to say that taking acetaminophen causes those behavioral or cognitive concerns.”
Some researchers do think the associations are worrisome enough to caution women taking acetaminophen during pregnancy. In 2021, an international group of scientists, clinicians, and public health professionals published what they called a “consensus statement” in Nature Reviews Endocrinology, which madenews for calling for “precautionary action” based on data indicating acetaminophen might alter fetal development, with an increasing impact with increasing duration of exposure.
“We recognize that limited medical alternatives exist to treat pain and fever; however, we believe the combined weight of animal and human scientific evidence is strong enough for pregnant women to be cautioned by health professionals against its indiscriminate use, both as a single ingredient and in combination with other medications,” the researchers wrote.
The statement proved controversial, however, with other groups of scientists pushing back to add context and explain why acetaminophen might not have caused the links seen in the studies.
“In my opinion, the level of evidence out there is poor, and I do not believe that there is any causal or any other association between at least short-term use of acetaminophen during pregnancy and ensuing increased risk of childhood ADHD or ASD [autism],” Dr. Per Damkier, a professor and clinical pharmacologist at Odense University Hospital and University of Southern Denmark, told us in an interview. Damkier was one of the scientists who pushed back at the consensus statement.
Multiple factors contribute to autism and ADHD. These conditions “are variable in clinical presentation, very difficult to assess and associate with a single causal factor,” Alwan said.
Damkier emphasized that many studies do not adequately take into account whether the parents had ADHD or autism, which run in families. He pointed to one study that suggested accounting for ADHD in parents likely weakens the relationship between this disorder and acetaminophen.
Many studies also rely on questionnaires filled out by parents, Damkier said. These may identify children at increased risk of ADHD or autism but do not replace an official diagnosis.
Finally, Damkier said that even if you accepted the analyses in the studies showing increased risk as valid, “which you should not,” the risk levels — typically 20% to 30% increased risk during childhood — represent a “weak association,” especially since there is typically a fair to moderate degree of uncertainty surrounding the numbers.
A Closer Look at Cord Blood
A 2019 JAMA Psychiatry study, which is cited in legaladvertisements, did not rely on self-reported data, instead looking at concentrations of broken down acetaminophen components in blood collected at Boston Medical Center from umbilical cords at birth and stored for future study.
The children with acetaminophen exposure in the top third — meaning the highest concentrations of the drug components in cord blood — had 2.86 times higher odds of an ADHD diagnosis and 3.62 times higher odds of an autism diagnosis compared with children with exposure in the bottom third. “Our findings support previous studies regarding the association between prenatal and perinatal acetaminophen exposure and childhood neurodevelopmental risk and warrant additional investigations,” the authors wrote.
The authors themselves noted some limitations of the paper at the time of publication. The cord blood measurements did not give a sense of acetaminophen exposure throughout pregnancy, instead showing recent use by people who had just given birth. Further, “caution is needed to apply our findings to other populations with different characteristics,” they wrote. Finally, one author pointed out in a press release that the study does not show that Tylenol causes ADHD or autism.
Damkier and others said that some observations and the characteristics of the children in the study appeared unusual, making it hard to draw general conclusions. Every cord blood sample showed acetaminophen exposure, he noted, and there were extremely high rates of ADHD and autism among the children. The study also lacked information on the mothers’ use of drugs or history of psychiatric disease.
Acetaminophen Treats Pain and Fever During Pregnancy
Expert groups said that acetaminophen can have benefits for pregnant people experiencing pain or fever, and there may not be good alternatives. The ACOG statement reads: “ACOG and obstetrician-gynecologists across the country have always identified acetaminophen as one of the only safe pain relievers for pregnant individuals during pregnancy.”
Nonsteroidal anti-inflammatory drugs, such as ibuprofen and aspirin, can have risks during pregnancy. Taking these drugs during later portions of pregnancy can lead to problems including insufficient amniotic fluid volume and premature closing of a major blood vessel in the fetus. Opioids can also harm the fetus and lead to withdrawal at birth, as well as pose risks for the mother.
Avoiding acetaminophen could have consequences for both mother and child. Fever early in pregnancy can lead to defects in the neural tube affecting the formation of the brain or spinal cord, Alwan said, noting that it is “critically important to treat fever in pregnancy.”
The Society for Maternal-Fetal Medicine statement calls acetaminophen “a reasonable and appropriate medication choice for the treatment of pain and/or fever during pregnancy.”
The authors of the 2021 Nature Reviews Endocrinology statement suggested doing more research into acetaminophen during pregnancy and cautioned women to “forego APAP [acetaminophen] unless its use is medically indicated; consult with a physician or pharmacist if they are uncertain whether use is indicated and before using on a long-term basis; and minimize exposure by using the lowest effective dose for the shortest possible time.”
This advice is in line with longstanding recommendations for pregnant people. “ACOG’s clinical guidance remains the same and physicians should not change clinical practice until definitive prospective research is done. Most importantly, patients should not be frightened away from the many benefits of acetaminophen. However, as always, any medication taken during pregnancy should be used only as needed, in moderation, and after the pregnant patient has consulted with their doctor,” the ACOG statement said.
“It is important for pregnant women and all women of reproductive age who may become pregnant to always consult their health care provider to find the best treatment option for pain or fever in pregnancy, which may be taking the recommended dose of acetaminophen and making sure to stay well hydrated and getting lots of rest,” Alwan said. People with questions about medications during pregnancy or breastfeeding can contact organizations like MotherToBaby, she added.
An FDA spokesperson told us in an email: “The FDA is aware of and understands the concerns arising from reports questioning the safety of prescription and over-the-counter (OTC) pain medicines when used during pregnancy. As a result, we evaluated research studies on acetaminophen published in the medical literature and determined that they are too limited to make any recommendations based on these studies at this time. Because of this uncertainty, the use of pain medicines during pregnancy should be carefully considered. We urge pregnant persons to always discuss all medicines with their health care professionals before using them. Acetaminophen labels contain the following information regarding pregnancy: ‘If pregnant or breast feeding, ask a health professional before use.’ The FDA continues to review the published literature and to monitor the potential impacts of acetaminophen.”
The spokesperson concluded by sharing a link to a 2015 Drug Safety Communication describing an FDA review of the risks of pain medicine during pregnancy. The document noted that severe and persistent pain, when not treated effectively, can lead to depression, anxiety and high blood pressure for the pregnant individual.
Correction, May 30: An earlier version of this article incorrectly stated that acetaminophen is an ingredient in oxycodone. Oxycodone is an opioid that is sometimes combined with acetaminophen. We thank the reader who brought this to our attention.
Clarification, June 6: An earlier version of this article listed drugs that contain acetaminophen, but did not make clear that acetaminophen is only in some versions of several of the drugs. We have updated the article to clarify this point. We thank the reader who brought this to our attention.
Editor’s note: SciCheck’s articles providing accurate health information and correcting health misinformation are made possible by a grant from the Robert Wood Johnson Foundation. The foundation has no control over FactCheck.org’s editorial decisions, and the views expressed in our articles do not necessarily reflect the views of the foundation.”
In my opinion as a acute nurse 37 years this topic needs much more research to put the blame only on Tylenol but for decades in general, drugs unless absolutely necessary should not be used during pregnancy because drugs taken by a pregnant woman can reach the fetus with side effects and be permanent possibly but in some cases it is necessary and not just Tylenol. The pregnant women is the one also to say if she will allow it. So the reason it was taken goes case by case. Ending line more research is needed. For example look at Covid and the vaccination with shutting down over a year, just saying.
Sources
Acetaminophen – ASD/ADHD Products Liability Litigation. MDL No. 3043. Transfer Order. United States Judicial Panel on Multidistrict Litigation. 5 Oct 2022.