Kurt Cobain (Former Lead Singer of Nirvana)
Archives
What is Scoliosis?
Scoliosis is a problem with the spine where the spine is curved instead of straight, with the upper back being rounded and the lower back having a “swayback,” or inner curved problem, reports WebMD.
According to the Scoliosis Research Society, 85 percent of all scoliosis causes are idiopathic, meaning the cause is unknown. The remaining causes of scoliosis include birth defects, such as vertebrae that form abnormally before birth, and certain disorders such as cerebral palsy, Marfan’s syndrome, muscular dystrophy and Down syndrome. Infections and spinal fractures can also cause scoliosis.curvature of the spine during surgical correction of this condition. Screws and rods are placed in order to stabilize and straighten the spine.
What You Should Know About Adult Scoliosis
Scoliosis is defined as a curve of the spine of 10 degrees. Adult scoliosis is broadly defined as a curve in your spine of 10 degrees or greater in a person 18 years of age or older. Adult scoliosis is separated into 2 common categories:
- Adult Idiopathic Scoliosis patients have had scoliosis since childhood or as a teenager and have grown into adulthood. We do not yet know the cause of idiopathic scoliosis, but there is a lot of genetic work going on in an attempt to answer this question.
- Adult “De Novo” or Degenerative Scoliosis develops in adulthood. Degenerative scoliosis develops as a result of disc degeneration. As the disc degenerates, it loses height. If one side of the disc degenerates more rapidly than the other, the disc begins to tilt. As it tilts, more pressure is placed on one side of your spine and gravity tends to cause the spine to bend and curve. The more discs that degenerate, the more the spine begins to curve.Types of idiopathic scoliosis are categorized by both age at which the curve is detected and by the type and location of the curve.
- When grouped by age, scoliosis usually is categorized into three age groups:
- Scoliosis is more common in girls than in boys, and the diagnosis is usually made after a child reaches 10 years of age. A doctor performs a physical examination and may take X-rays to definitively diagnose the disease. An X-ray tells if there is any growth left in the growth plates of the femur or humerus, and scoliosis can become worse if the patient has more growing to do, states MedicineNet. Serial X-rays are performed to track the changes of the spinal curve, which helps determine the best course of treatment.
- Infantile scoliosis: from birth to 3 years old
- Juvenile scoliosis: from 3 to 9 years old
- Adolescent scoliosis: from 10 to 18 years oldTerms Used to Describe Spinal CurvatureTerms that describe the direction of the curve:
- Scoliosis curves are often described based on the direction and location of the curve. Physicians have several detailed systems to classify specific curves, but here are some common terms used to describe scoliosis:
- This last category of scoliosis, adolescent scoliosis, occurs in children age 10 to 18 years old, and comprises approximately 80% of all cases of idiopathic scoliosis. This age range is when rapid growth typically occurs, which is why the detection of a curve at this stage should be monitored closely for progression as the child’s skeleton develops.
- Dextroscoliosis describes a spinal curve to the right (“dextro” = right). Usually occurring in the thoracic spine, this is the most common type of curve. It can occur on its own (forming a “C” shape) or with another curve bending the opposite way in the lower spine (forming an “S”).Symptoms of scoliosis include an uneven waist, uneven shoulders, disjointed hip and a protruding shoulder blade, according to Mayo Clinic. The spine also curves or twists in acute cases, and the disease can cause one side of the ribs to protrude more than the other. Severe cases also induce labored breathing and back pain.Scoliosis can be recognized and diagnosed with a clinical exam, but xrays are necessary to fully evaluate the magnitude and type of scoliosis present. For a proper scoliosis evaluation, full length, whole spine xrays need to be performed. An MRI may also be recommended if there are symptoms of leg pain that may be associated with stenosis or if there is concern about possible spinal cord compression or abnormalities.The treatment of adult scoliosis is very individualized and based on the specific symptoms and age of the patient. Many patients have scoliosis and have very minor symptoms and live with it without treatment. Patients with predominant symptoms of back pain would typically be treated with physical therapy. Patients with back pain and leg pain may receive some benefit from injection treatment to help relieve the leg pain. If lumbar stenosis (narrowing of the spinal canal) is present and is unresponsive to non-surgical treatment, then a decompression( removal of bone and ligaments pressing on the nerves) may be recommended. If the scoliosis is greater than 30 degrees, a fusion procedure will most likely be recommended along with the decompression. The fusion is recommended to prevent the curve from progressing when the spine is destabilized by the bone removal that is necessary to decompress the nerves. Fusions are usually accompanied with metal rod and screw placement into the spine to help correct and stabilize the scoliosis and help the bone heal or fuse together. The length of the fusion, or the number of spine levels included, depends on the type of scoliosis and the area of the spine involved. The goal of adult scoliosis surgery is to first remove pressure on the nerves, and second to keep the scoliosis from progressing further.
- Treatment
- Diagnosis
- Severe scoliosis can lead to heart and lung problems if not treated, as the ribs press against the chest, making breathing more difficult, states Mayo Clinic. Adults who had scoliosis as a child may experience more back pain throughout their lives as compared to people without scoliosis.
QUOTE FOR THURSDAY:
“An estimate that 50 percent of men in their 50s have an enlarged prostate. The prostate is the gland that produces the fluid that carries sperm. It grows larger with age.”
The Urology Care Foundation
BPH-Benign Prostatic Hypertrophy or Hyperplasia.
The prostate is a walnut-shaped gland that is part of the male reproductive system. The main function of the prostate is to make a fluid that goes into semen. Prostate fluid is essential for a man’s fertility. The gland surrounds the urethra at the neck of the bladder. The bladder neck is the area where the urethra joins the bladder. The bladder and urethra are parts of the lower urinary tract. The prostate has two or more lobes, or sections, enclosed by an outer layer of tissue, and it is in front of the rectum, just below the bladder. The urethra is the tube that carries urine from the bladder to the outside of the body. In men, the urethra also carries semen out through the penis.
What is benign prostatic hyperplasia?
Benign prostatic hyperplasia––also called BPH––is a condition in men in which the prostate gland is enlarged and not cancerous. Benign prostatic hyperplasia is also called benign prostatic hypertrophy or benign prostatic obstruction.
The prostate goes through two main growth periods as a man ages. The first occurs early in puberty, when the prostate doubles in size. The second phase of growth begins around age 25 and continues during most of a man’s life. Benign prostatic hyperplasia often occurs with the second growth phase.
As the prostate enlarges, the gland presses against and pinches the urethra. The bladder wall becomes thicker. Eventually, the bladder may weaken and lose the ability to empty completely, leaving some urine in the bladder. The narrowing of the urethra and urinary retention––the inability to empty the bladder completely––cause many of the problems associated with benign prostatic hyperplasia.
Ending line the prostate enlarges pushes up to the superior both front and back aspects of the penis (just below the urinary bladder) narrowing the urethra in the penis shaft (on both sides of the urethra) causing urination difficulty and frequently urinating. (See figure below the picture shows in the top part the urinary bladder and the prostate below it Left normal Right BPH).
What causes benign prostatic hyperplasia?
The cause of benign prostatic hyperplasia is not well understood; however, it occurs mainly in older men. Benign prostatic hyperplasia does not develop in men whose testicles were removed before puberty. For this reason, some researchers believe factors related to aging and the testicles may cause benign prostatic hyperplasia.
Throughout their lives, men produce testosterone, a male hormone, and small amounts of estrogen, a female hormone. As men age, the amount of active testosterone in their blood decreases, which leaves a higher proportion of estrogen. Scientific studies have suggested that benign prostatic hyperplasia may occur because the higher proportion of estrogen within the prostate increases the activity of substances that promote prostate cell growth.
Another theory focuses on dihydrotestosterone (DHT), a male hormone that plays a role in prostate development and growth. Some research has indicated that even with a drop in blood testosterone levels, older men continue to produce and accumulate high levels of DHT in the prostate. This accumulation of DHT may encourage prostate cells to continue to grow. Scientists have noted that men who do not produce DHT do not develop benign prostatic hyperplasia.
How common is BPH?
Benign prostatic hyperplasia is the most common prostate problem for men older than age 50. In 2010, as many as 14 million men in the United States had lower urinary tract symptoms suggestive of benign prostatic hyperplasia. Although benign prostatic hyperplasia rarely causes symptoms before age 40, the occurrence and symptoms increase with age. Benign prostatic hyperplasia affects about 50 percent of men between the ages of 51 and 60 and up to 90 percent of men older than 80.
Signs and Symptoms
BPH, the prostate gland grows in size. It may compress the urethra which courses through the center of the prostate. This can impede the flow of urine from the bladder through the urethra to the outside. It can cause urine to back up in the bladder (retention) leading to the need to urinate frequently during the day and night. Other common symptoms include a slow flow of urine, the need to urinate urgently and difficulty starting the urinary stream. More serious problems include urinary tract infections=pain in pelvic region and complete blockage of the urethra, which would be a medical emergency and can lead injury to the kidneys.
Treatment:
Is BPH always treated?
No. Treatment of BPH is usually reserved for men with significant symptoms. Watchful waiting with medical monitoring once a year is appropriate for most men with BPH.
How is BPH treated?
There are several different ways to treat BPH:
Men should carefully weigh the risks and benefits of each of these options. Prostate surgery has traditionally been seen as offering the most benefits for BPH but unfortunately carries the most risks.
- Watchful waiting is often chosen by men who are not bothered by symptoms of BPH. They have no treatment but get regular checkups and wait to see whether or not the condition gets worse.
Medical Treatment through drugs is used by some men rangaing from alpha blockers relax the smooth muscles of the prostate, and the bladder neck. An example of these meds are tamsulosin (Flomax), alfuzosin (Uroxatral), and older medications such as terazosin (Hytrin), slidosin (Rapaflo) or doxazosin (Cardura).
Also 5-alpha reductase inhibitors block the conversion of the male hormone testosterone into its active form in the prostate. Examples of 5-alpha reductase inhibitors include Finasteride (Proscar) and dutasteride (Avodart). Side effects of finasteride may include declining interest in sex, problems getting an erection, and problems with ejaculation.
Surgery or office procedures may also be used to treat BPH, most commonly in men who have not responded satisfactorily to medication or those who have more severe problems, such as a complete inability to urinate.
- Transurethral resection of the prostate (TURP) has been used for the longest period of time. After the patient is given anesthesia, the doctor inserts a special instrument into the urethra through the penis. With the instrument, the doctor then shaves away part of the inner prostate to relieve the outflow of urine from the bladder.
- Laser procedures: A number of laser procedures are available, some of which can be performed in the doctor’s office with minimal anesthesia. These procedures also involve the removal of obstructing prostate tissue. They are generally associated with less bleeding and quicker recovery than TURP.
- Microwave therapy: This procedure is generally performed in the office and involves the use of microwave energy delivered to the prostate to kill some of the cells leading eventually to shrinkage of the prostate.
QUOTE FOR WEDNESDAY:
“In hemodialysis, your blood is allowed to flow, a few ounces at a time, through a special filter that removes wastes and extra fluids including harmful wastes. The clean blood is then returned to your body.”
The National Institute of Diabetes & Digestive and Kidney Disease.
Dialysis

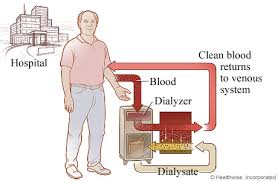
Dialysis is a treatment for kidney failure that removes waste and extra fluid from the blood, using a filter. In hemodialysis (HD), the filter is a plastic tube filled with millions of hollow fibers, called a dialyzer. Hemodialysis is the most common way to treat advanced kidney failure. The procedure can help you carry on an active life despite failing kidneys. Hemodialysis requires you to follow a strict treatment schedule, take medications regularly and, usually, make changes in your diet. Hemodialysis is a serious responsibility, but you don’t have to shoulder it alone. You’ll work closely with your health care team, including a kidney specialist and other professionals with experience managing hemodialysis. You may be able to do hemodialysis at home. Peritoneal (per-ih-toe-NEE-ul) dialysis is another way to remove waste products from your blood when your kidneys can no longer do the job adequately. During peritoneal dialysis, blood vessels in your abdominal lining (peritoneum) fill in for your kidneys, with the help of a cleansing fluid that flows into and out of the peritoneal space.
Hemodialysis is typically conducted in a dedicated facility with specialized nurses and technicians who specialize in hemodialysis. However, dialysis can also be done in a patient’s home. Once you and your doctor have determined that at home hemodialysis is right for you, you will begin a comprehensive safety and training program that is tailored to your specific medical and learning needs.
In most cases, you will learn to perform at home hemodialysis treatments with a dialysis partner. An access will have to be created to allow blood to flow from your body to the dialyzer, so it can filter waste and remove extra fluid from your body. There are different ways to create an access, and you will discuss with your doctor which one is right for you and your treatment.
There are three types of at home hemodialysis:
- Short Daily at Home Hemodialysis – Performed five or six times a week, typically for two to three hours per session.
- Traditional at Home Hemodialysis – Performed three times per week, typically for about four hours per session. This is similar to the treatments received at a local dialysis center.
- Nocturnal Home Hemodialysis – Performed during sleep, typically six to eight hours a night, three or more nights a week. Many patients enjoy the ability to spend the night dialyzing and not lose time during the day that could be spent at work or with family.
When is dialysis needed?
You need dialysis if your kidneys no longer remove enough wastes and fluid from your blood to keep you healthy. This usually happens when you have only 10 to 15 percent of your kidney function left. You may have symptoms such as nausea, vomiting, swelling and fatigue. However, even if you don’t have these symptoms yet, you can still have a high level of wastes in your blood that may be toxic to your body. Your doctor is the best person to tell you when you should start dialysis.
How long will each hemodialysis treatment last?
In a dialysis center, hemodialysis is usually done 3 times per week for about 4 hours at a time. People who choose to do hemodialysis at home may do dialysis treatment more frequently, 4-7 times per week for shorter hours each time.
Your doctor will give you a prescription that tells you how much treatment you need. Studies have shown that getting the right amount of dialysis improves your overall health, keeps you out of the hospital and enables you to live longer. Your dialysis care team will monitor your treatment with monthly lab tests to ensure you are getting the right amount of dialysis. One of the measures your dialysis care team may use is called urea reduction ratio (URR). Another measure is called Kt/V (pronounced kay tee over vee). Ask your dialysis care team what measure they use and what your number is. To ensure that you are getting enough dialysis:
- *your Kt/V should be at least 1.2 or
- *your URR should be at least 65 percent.
Can I have hemodialysis at home?
Possibly. Many patients have their hemodialysis treatments at home. The doctor will let you know if that is ideal for your state of kidney failure and where you are at for your optimal level of treatment.
Do I need to eat a special diet?
Yes. Generally speaking, patients on dialysis are advised to increase their protein intake and limit the amount of potassium, phosphorus, sodium, and fluid in their diet. Patients with diabetes or other health conditions may have additional diet restrictions. It’s important to talk with you dietitian about your individual diet needs.
Your dialysis care team will monitor your treatment with monthly lab tests to ensure you get the right amount of dialysis and that you are meeting your dietary goals.
Can dialysis cure my kidney disease?
In some cases of sudden or acute kidney failure, dialysis may only be needed for a short time until the kidneys get better. However, when chronic kidney disease progresses to kidney failure over time, your kidneys do not get better and you will need dialysis for the rest of your life unless you are able to receive a kidney transplant.
Will I be uncomfortable on hemodialysis?
When you begin hemodialysis, the needles put in your fistula or graft may be uncomfortable. Most patients get used to this in time. Your dialysis care team will make sure you are as comfortable as possible during your treatment. Symptoms like cramps, headaches, nausea or dizziness are not common, but if you do have any of them, ask your dialysis care team if any of the following steps could help you:
- *Slow down your fluid removal, which could increase your dialysis time.
- *Increase the amount of sodium in your dialysate.
- *Check your high blood pressure medications.
- *Adjust your dry weight, or target weight.
- *Cool the dialysate a little.
- *Use a special medication to help prevent low blood pressure during dialysis.
You can help yourself by following your diet and fluid allowances. The need to remove too much fluid during dialysis is one of the things that may make you feel uncomfortable during your treatment.
Can dialysis cure my kidney disease?
In some cases of sudden or acute kidney failure, dialysis may only be needed for a short time until the kidneys get better. However, when chronic kidney disease progresses to kidney failure over time, your kidneys do not get better and you will need dialysis for the rest of your life unless you are able to receive a kidney transplant.
QUOTE FOR TUESDAY:
According to experts at NIH, the two most common causes of kidney disease are diabetes and high blood pressure. If your family has a history of any kind of kidney problems, you may be at risk for kidney disease.
National Institute of Health
QUOTE FOR MONDAY:
“Many times this is reversible but depending on the cause and severity, it may be irreversible and lead to chronic renal failure or chronic kidney disease.”
MedicineNet.com
PART1 ACUTE RENAL FAILURE VERSUS CHRONIC RENAL FAILURE
Acute Renal (Kidney) Failure:
Kidney failure occurs when the kidneys lose their ability to function. To treat kidney failure effectively, it is important to know whether kidney disease has developed suddenly (acute) or over the long term (chronic). Many conditions, diseases, and medicines can create situations that lead to acute and chronic kidney disease. Acute kidney injury, also called acute renal failure, is more commonly reversible than chronic kidney failure since the chronic condition has lasted longer in the body affecting systems for several months to years (some decades). Acute Renal Failure is new to the body as opposed to chronic; making it higher odds this can be treated and cured.
When acute kidney injury occurs, the kidneys are unable to remove waste products and excess fluids, which then build up in the body and upset the body’s normal chemical balance.*
The most common causes of acute kidney injury are:
-dehydration
-blood loss from major surgery or injury
-medicines such as nonsteroidal anti-inflammatory drugs (NSAIDs), antibiotics, or the dyes (contrast agents) used in X-ray tests.
Symptoms depend on the cause of the problem of acute renal failure and can include:
- -Little or no urine output.
- -Dizziness upon standing.
- -Swelling, especially of the legs and feet.
- -Loss of appetite, nausea, and vomiting.
- -Feeling confused, anxious and restless, or sleepy.
- -Pain in the flank, which is felt just below the rib cage and above the waist on one or both sides of the back.* Further your doctor will do the following to diagnose the condition other than blood tests:
- Most cases of acute kidney injury occur in people who are already in the hospital for other reasons. In these people, acute kidney injury is usually diagnosed when routine tests show a sudden increase in creatinine and blood urea nitrogen (BUN) levels. A buildup of these waste products in the blood points to a loss of kidney function.
- -Your doctor will compare these levels to previous tests to find out if kidney disease is acute or chronic.
- -Also commonly done is an ultrasound of the kidneys which may help determine whether kidney problems are acute or chronic. Normal-sized kidneys may be present in either condition, but when both kidneys are smaller than normal, chronic kidney disease is usually the problem. This helps rule out acute from chronic.–correcting the cause and supporting the kidneys with dialysis until proper functioning is restored. Most people who develop acute kidney injury are already in the hospital.In giving a short and easily understandable definition Chronic kidney disease happens when your kidneys no longer filter your blood the way they should, so wastes (toxins, usually end products of an acid) build up in your blood. This has probably been going on for years, and it may keep getting worse over time. Just like a car engine damaged but still using the car without getting the engine repaired sooner or later in time the engine no longer functions the same with any organ of the body getting damaged by some long term condition. If your disease gets worse and worse over time, you could have kidney failure for some multi organ failure, depending on the condition causing this.*-Diabetes (uncontrolled diabetes (Type 1 or 2) for many years. *-High blood pressure for many years. These are the top 2 causes of most chronic kidney disease. Controlling these diseases can help slow or stop the damage to the individual’s kidneys who has one of these, if not both.-A narrowed or blocked renal artery. A renal artery carries blood to the kidneys.Know this for starters, each of your kidneys has about a million tiny filters, called nephrons.The nephron is the tiny filtering structure in your kidneys. Each of your kidneys contain more than a million tiny filtering nephrons that help clean your blood removing toxins dumping them into your urinary bladder so you can evacuate them though urine (urea, urine; get it). Your nephrons play a vital role to our essential daily living. They help all humans do the following if there kidneys or one kidney is functioning properly. They:
- -Long-term use of medicines that can damage the kidneys. Examples include nonsteroidal anti-inflammatory drugs (NSAIDs), such as celecoxib and ibuprofen.
- Other causes that can lead to chronic kidney disease include: -Kidney diseases and infections, such as polycystic kidney disease, pyelonephritis, and glomerulonephritis, or a kidney problem you were born with.
- The most common causes of Chronic Renal Failure are:
- Chronic Renal (Kidney) Failure:
- The treatment of acute kidney injury includes:
- -Remove excess water, wastes (like urea, ammonia, etc.) & other substances from your blood.
- -Return substances like sodium, potassium or phosphorus whenever any of these substances run low in your body.
- If nephrons are damaged by the high sugar content or high blood pressure in the kidneys, they stop working. For a while, healthy nephrons can take on the extra work or overload. But if the damage continues, more and more nephrons shut down. After a certain point, the nephrons that are left cannot filter your blood well enough to keep you’re blood filtered properly to keep you healthy. Just like running from a bear in the street chancing you. We can run only so long but sooner or later we will run out of energy and not be able to run anymore, same concept for the kidney nephrons when they run out of enough not properly working.
QUOTE FOR THE WEEKEND:
“The general population has about a 1% risk of developing epilepsy. Meanwhile, children of mothers with epilepsy have a 3 to 9% risk of inheriting this disease, while children of fathers have a 1.5 to 3% risk of inheritence.” Based on genes research
Dr. Robert S. Fischer Ph D. Stanford Epilepsy Center http://neurology.stanford.edu/epilepsy/patientcare/videos