“When you exhaust all possibilities remember this: You haven’t!”
Thomas Edison (Inventor and Businessman)
“When you exhaust all possibilities remember this: You haven’t!”
Thomas Edison (Inventor and Businessman)
“But the key to our marriage is the capacity to give each other a break. And to realize that it’s not how our similarities work together; it’s how our differences work together.”
Michael J. Fox (Actor & spokesman for Parkinson’s Disease)
How to care for IBS:
1. IBS Treatment through Diet
2. IBS Treatment through Supplements
3. IBS Treatment through Alternative Therapies
4. IBS Treatment through Stress Management
5. IBS Treatment through Prescription Medications
Help from IBS.com
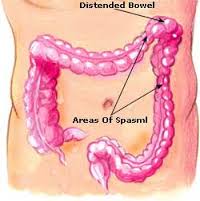
Irritable bowel syndrome is a group of symptoms – including abdominal pain and changes in the pattern of bowel movements without any evidence of underlying damage. These symptoms occur over a long time, often years. It has been classified into four main types depending on if diarrhea is common, constipation is common, both are common, or neither occurs very often. IBS negatively affects quality of life and may result in missed school or work. Disorders such as anxiety, major depression, and chronic fatigue syndrome, are common among people with IBS.
Treatments and drugs
Because it’s not clear what causes irritable bowel syndrome, treatment focuses on the relief of symptoms so that you can live as normally as possible.
In most cases, you can successfully control mild signs and symptoms of irritable bowel syndrome by learning to manage stress and making changes in your diet and lifestyle. Try to avoid foods that trigger your symptoms. Also try to get enough exercise, drink plenty of fluids and get enough sleep.
If your problems are moderate or severe, you may need more than lifestyle changes. Your doctor may suggest medications.
Dietary changes:
“A study just published by Clinicians on patients in the West Midlands who travelled overseas to receive Living Donor transplants has found that clinical outcomes are often poor. Over 30% of the patients in the study who travelled either died within three months (17%) or lost their new kidney within a year(14%).”
National Kidney Federation
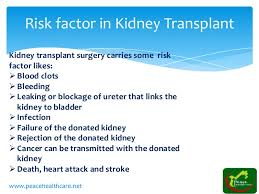
When people languish on a wait-list for a kidney transplant, they may start to consider a desperate measure: Traveling to a country where they can buy a donor kidney on the black market.
But beyond the legal and ethical pitfalls, experts say, the health risks are not worth it.
Most countries ban the practice, sometimes called “transplant tourism,” and it has been widely condemned on ethical ground. Now a new study highlights another issue: People who buy a donor kidney simply do not fare as well.
Researchers in Bahrain found that people who traveled abroad to buy a kidney — to countries like the Philippines, India, Pakistan, China and Iran — sometimes developed serious infections.
Those infections included the liver diseases hepatitis B and C, as well as cytomegalovirus, which can be life-threatening to transplant recipients, the investigators said.
Also, people who bought donor kidneys also faced higher rates of surgical complications and organ rejection, versus those who received a legal transplant in their home country.
Dr. Amgad El Agroudy, of Arabian Gulf University, was to present the findings Friday at the annual meeting of the American Society of Nephrology (ASN), in San Diego.
It’s not clear how common it is for U.S. patients to take a chance on traveling abroad to buy a black-market kidney, according to Dr. Gabriel Danovitch, director of kidney transplantation at the University of California, Los Angeles.
“We really have no way of knowing what the numbers are,” said Danovitch, who was not involved in the study.
“But,” he added, “my sense is that the numbers are fairly small, as the dangers of transplant tourism are becoming more and more clear.”
Why is it a risky proposition? According to Danovitch, there are a few broad reasons: The paid organ donors may not be properly screened, and the recipients may not be good candidates for a transplant, to name two.
“In a paid system, the prime focus is on making money,” Danovitch said. “Centers that are willing to do these don’t really care what happens to the donors or recipients after the transplant.”
For people with advanced chronic kidney failure, the treatment options are dialysis or a transplant. But there are not enough donor organs to meet the need. In the United States, nearly one million people have end-stage kidney disease, and there are roughly 102,000 people on the waiting list for a transplant, according to the National Kidney Foundation.
Kidney transplants can come from a living or deceased donor, but living-donor transplants are more likely to be successful, according to U.S. health officials.
It doesn’t take long to get tired of spending 12 hours a week on hemodialysis, or even more time on peritoneal dialysis (PD) —not to mention complications like line infections and access problems. But a new, healthy kidney would put an end to all that. A transplant sounds like it would be well worth the risk of surgery and the trouble of taking anti-rejection medicines, and Medicare statistics show that it actually costs less in the long run than continued dialysis. When can you check into the hospital, you ask?
Unfortunately over 80,000 people in the United States are already waiting for a new kidney and in 2008 only 16,517 got one. Maybe you don’t have a compatible donor in your family, or you’ve been told that you are “not a transplant candidate” for one of several reasons. You’re a resourceful person who knows that persistence pays off, and you start looking for ways to shorten the wait or get around the rules that say you don’t qualify for a transplant. Kidneys from living donors are almost always preferable to those from recently deceased donors. If you don’t have a friend or family member willing to donate, what about getting one where the laws against buying an organ are less strictly enforced? Medical tourism is booming these days. Maybe you know somebody who had surgery overseas, either to avoid a waiting list or just because the price is lower there. The same international pharmaceutical countries produce medicines for everybody these days, so how big a difference can there be? Nephrologists in the US say it’s a common story: a dialysis patient misses treatments or appointments for a few days or several weeks, then comes to their office asking for refills on anti-rejection medicines…with pill bottles labeled in Urdu, Chinese or Farsi as well as in English. Did they get a good deal or what? Unfortunately this may not be the bargain people hoped for.
At UCLA Jagbir Gill, MD, and associates studied 33 patients who had received transplants overseas, and found they had much worse results than patients who received transplants in this country. Screening of paid kidney donors was less thorough, with problems like hepatitis overlooked. Early organ rejection was twice as common and infections frequent; Dr. Gill recalls patients who went “directly from the airport to the emergency room” due to severe infections or transplant failure.
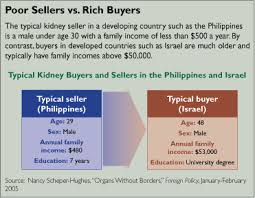
In a similar study in Canada, where waiting periods for transplants are even longer, experiences were similar. Jeffrey Zaltzman, MD, reports infections common in the countries where the transplant was done were a big problem in medical tourists. One 78-year-old gentleman returned from Pakistan with a surgical wound that reopened spontaneously; he died a few weeks later of cardiovascular problems that might have disqualified him for a transplant at home. The cost to paid organ donors can be even greater. Poor people who sell a kidney, sometimes for as little as $800 according to the World Health Organization, face health problems like hypertension and worsening of their own kidney functions—provided, of course, that their surgery goes well. Since most live in countries where even blood pressure checks are rare, complications that develop after they leave the hospital may go undetected until it is too late for the patient. Donors in the United States frequently can have kidneys removed with very small incisions. Third World donors, however, generally end up with wounds up to 14 inches long that may take months to heal, making them unable to do the manual labor most depend on. Chronic pain and disability are common, points out Nancy Scheper-Hughes, who has extensively studied and reported on transplant practices from Brazil to China. And reports of organs coming from executed prisoners in China are even more worrisome. Details of where donors come from and which hospitals and doctors will do the surgery are rarely available to “clients” and their families ahead of time. While paying a donor for an organ is illegal everywhere except Iran, “international transplant coordinators” have no laws banning what they do—bringing clients together with hospitals in other countries. And as the WHO’s Dr. Luc Noel points out, “None of the brokers ever mention the costs—long-term health issues, chronic pain, inability to perform manual labor—that are borne by these poor organ vendors.”
SO THINK TWICE BEFORE FALLING FOR TRANSPLANT TOURISM. HIGH PROBABILITY YOU WON’T LIKE THE RESULTS!
“2 ways to replace the kidneys: Hemodialysis cleans and filters your blood using a machine to temporarily rid your body of harmful wastes, extra salt, and extra water. Hemodialysis helps control blood pressure and helps your body keep the proper balance of important chemicals such as potassium, sodium, calcium, and bicarbonate. Peritoneal dialysis is another procedure that removes wastes, chemicals, and extra water from your body. This type of dialysis uses the lining of your abdomen, or belly, to filter your blood.”
National Institute of Diabetes and Digestive and Kidney Diseases
There is not always a simple easy answer for a patient that has chronic renal disease regarding which choice or option of dialysis that is best for him or her ; so let’s investigate the options & know you can always change the choice of dialysis you initially go on. But remember you are going from a tube placed in your circulatory system to a tube now in your abdomen or visa versa (depending on what your first choice of diaysis was) and that both tubes take time to be ideally ready and final for dialysis after inserted. So definitely take consideration in your choice both for your body and time it takes to allow the tube (especially in hemodialysis) in getting at its optimal level or state in being used:
| Advantages | Limitations | |
| Peritoneal Dialysis | ·Flexible lifestyle and independence.
-Time commitment: usually less than 10 hrs per week -Time allotment: as per patient convenience -No needles -Simple techniques: easy learning -Continuous therapy: minimal fluctuation of symptoms -Once a month clinic, so no need to travel repeatedly -Easy personal travel, pack bags and go -Can use APD: connect at night and go to sleep |
Limitations are you need to weave this into lifestyle
-Abdominal catheter -Does have passive sugar intake, so need to watch for weight gain -Needs storage space of around half a closet (supplies) |
| Home Hemodialysis | -Flexible lifestyle and independence
-Time commitment: based on therapy ~ 22 hours a week -Time allotment: at patient convenience -5-6 times a week so less symptomatic fluctuations -Much higher freedom in dietary and fluid intake -May eliminate the need for BP and some of the other medications -Easy to travel with, pack and go.. |
-Needs a caregiver at least for the duration of dialysis 5-6 times a week
-Higher commitment compared to hemodialysis -Need to weave into lifestyle -Needs storage space of around half a closet -Does need AVF creation and needle access |
| In Center Hemodialysis | -Dialysis done at clinic by dialysis technicians and nurses |
-Rigid schedule, limited flexibility -Time commitment: ~20 hours a week -Time allotment: no flexibility, as per dialysis unit -Need prior authorization and arrangement for travel -Cannot travel to region not having dialysis clinic -Significant fluctuation of symptoms -Does need AVF creation and needle access -Need transportation arrangements |
More than 1/2 a million patients in USA suffer from stage V CKD commonly referred to as Renal Failure (or End Stage Renal Disease (ESRD)) with nearly similar number of patients suffering with the pre-dialysis, stage IV CKD. The management of ESRD involves either replacement of the lost kidney function through the kidney transplantation, or clearing body of the accumulating toxins through maintenance dialysis. Unfortunately, kidney transplantation is not a viable option for a majority of ESRD patients due to a limited availability of donor organs, further compounded by the fact that many of the dialysis patients are medically unsuitable for transplantation. Thus, maintenance dialysis forms mainstay of the treatment for this large majority of the ESRD patients.
It is uniformly agreed that no single type of dialysis (home Vs In-center dialysis, or Hemo Vs peritoneal dialysis) is superior to others in terms of hard clinical endpoints e.g. mortality or cardiovascular deaths. However, home dialysis modalities (both PD and HHD) provide significant advantages in multiple outcome parameters important to the management of patients with ESRD namely quality of life, freedom of travel, greater liberty from dietary restrictions, preservation of residual kidney function etc.
Historically, analyses of various patient cohorts in US have consistently revealed that; a privileged patient cohort more frequently chooses a home dialysis. This in many circumstances have been reflected by higher use of peritoneal dialysis in patients that are Caucasians, patients with higher education, patient under the care of nephrologists during the pre-ESRD period, patients receiving pre-dialysis education etc. In fact, nearly half of the patients when provided with a comprehensive pre-dialysis education (CPE) opt for home dialysis. Additionally both individual kidney physician surveys and recommendations of various professional medical societies now recommend a higher utilization of home dialysis. Despite these, only a minority of ESRD patients in US are on Home dialysis modalities. Lack of patient awareness due to lack of pre-dialysis education and scarcity of medical experts performing the home dialysis therapies are the two principle reasons for this underutilization of Home dialysis therapies.
Considering these facts, University of Florida and DCI have established a specialized clinic and education set up where a comprehensive pre-dialysis education (CPE) will be provided to the patients with stage IV (pre-dialysis) CKD along with their multispecialty care for various ailments of CKD. This clinic will put a special emphasis on the comprehensive care of CKD patients with special attention towards their dietary needs, their social and pharmacological concerns and their awareness and needs for decision making for their eventual dialysis or transplant therapies.
In conclusion of renal failure and if you are chronic, it’s not always easy to decide which type of treatment is best for you. Your decision depends on your medical condition, lifestyle, and personal likes and dislikes.
**Discuss the pros and cons of each with your health care team. If you start one form of treatment and decide you’d like to try another, talk it over with your doctor. The key is to learn as much as you can about your choices. With that knowledge, you and your doctor will choose a treatment that suits you best.**
I hope this article help you in some small way or more in dealing with your chronic renal failure. Know your not alone and have many sites and places in giving you direction and support!
| Always do a Comparison of dialysis methods : Hemodialysis and Peritoneal dialysis: |
| What is usually involved | HEMODIALYSIS
|
PERITONEAL DIALYSIS
|
| Advantages |
|
|
| Disadvantages |
|
|
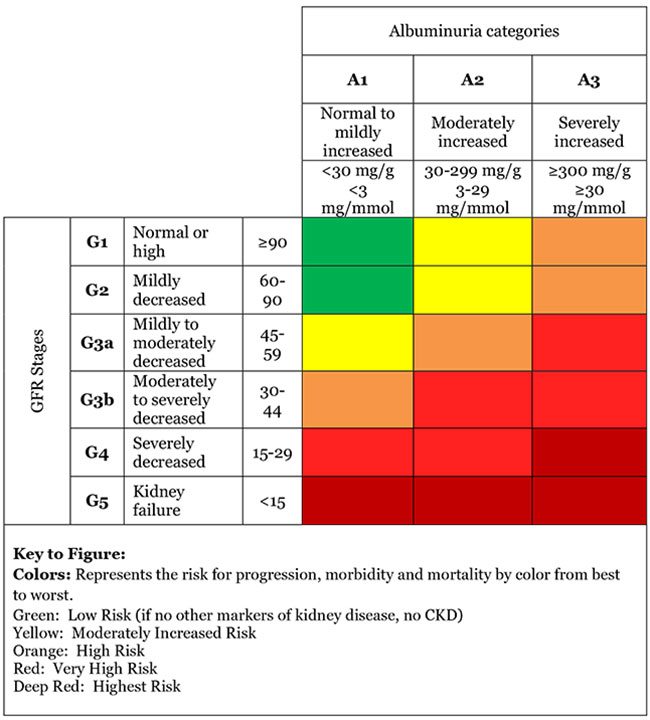
“The stages of CKD (Chronic Kidney Disease) are mainly based on measured or estimated GFR (Glomerular Filtration Rate). There are five stages but kidney function is normal in Stage 1, and minimally reduced in Stage 2.”
The Renal Association (founded 1950)
________________________________________________
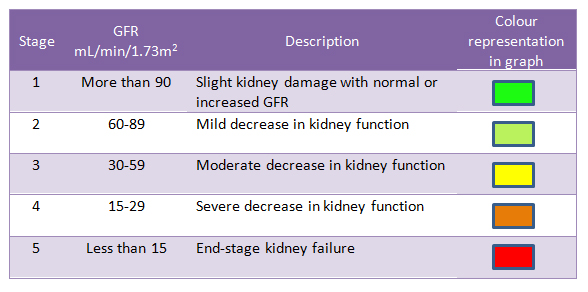
GFR – glomerular filtration rate is the best test to measure your level of kidney function and determine your stage of kidney disease. Your doctor can calculate it from the results of your blood creatinine test, your age, body size and gender. Your GFR tells your doctor your stage of kidney disease and helps the doctor plan your treatment. If your GFR number is low, your kidneys are not working as well as they should. The earlier kidney disease is detected, the better the chance of slowing or stopping its progression.
| Stage | Description | (GFR) |
| At increased risk | Risk factors for kidney disease (e.g., diabetes, high blood pressure, family history, older age, ethnic group) | More than 90 |
| 1 | Kidney damage with normal kidney function | 90 or above |
| 2 | Kidney damage with mild loss of kidney function | 89 to 60 |
| 3a | Mild to moderate loss of kidney function | 59 to 44 |
| 3b | Moderate to severe loss of kidney function | 44 to 30 |
| 4 | Severe loss of kidney function | 29 to 15 |
| 5 | Kidney failure | Less than 15 |
| Your GFR number tells you how much kidney function you have. As kidney disease gets worse, the GFR number goes down. | ||
What happens if my test results show I may have chronic kidney disease?
| Age (years) | Average estimated GFR |
| 20–29 | 116 |
| 30–39 | 107 |
| 40–49 | 99 |
| 50–59 | 93 |
| 60–69 | 85 |
| 70+ | 75 |
Follow a diet that is easy on your kidneys. A dietitian can help you make an eating plan with the right amounts of salt (sodium) and protein. You may also need to watch how much fluid you drink each day.
Make exercise a routine part of your life. Work with your doctor to design an exercise program that is right for you.
Do not smoke or use tobacco.
Do not drink alcohol.
When kidney function falls below a certain point, it is called Kidney failure. Kidney failure affects your whole body. It can cause serious heart, bone, and brain problems and make you feel very ill. Untreated kidney failure will be life-threatening at some point.
When you have kidney failure, you will probably have two choices: start dialysis or get a new kidney (transplant). Both of these treatments have risks and benefits. Talk with your doctor to decide which would be best for you.
Always talk to your doctor before you take any new medicine, including over-the-counter remedies, prescription drugs, vitamins,or herbs. These can hurt the kidneys further.
In COMPLETE RENAL FAILURE you have 2 choices for Rx.:
1**-Dialysis is a process that filters your blood when your kidneys no longer can. It is not a cure, but it can help you feel better and live longer. There is hemodialysis or peritoneal dialysis.
2-**Kidney transplant may be the best choice if you are otherwise healthy. With a new kidney, you will feel much better and will be able to live a more normal life. But you may have to wait for a kidney that is a good match for your blood and tissue type. And you will have to take medicine for the rest of your life to keep your body from rejecting the new kidney.
John for your knowledge – Westchester Medical Center enjoys a long and illustrious history in kidney transplantation, having performed well over 2100 kidney transplants since the program opened in 1989.
Making treatment decisions when you are very ill is hard! It is normal to be worried and afraid. Discuss your concerns with your loved ones and your doctor. It may help to visit a dialysis center or transplant center and talk to others who have made these choices.