“The major source of lead poisoning among U.S. children is lead-based paint and dust with lead.”
MAYO CLINIC
“The major source of lead poisoning among U.S. children is lead-based paint and dust with lead.”
MAYO CLINIC
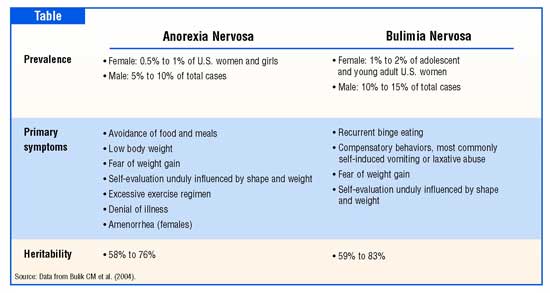
“Anorexia nervosa and bulimia nervosa are serious psychiatric illnesses related to disordered eating and distorted body images. They both have significant medical complications associated with the weight loss and malnutrition.”
Science Direct
Medical Complications of Anorexia Nervosa:
Low heart rate, low body temperature, low blood pressure, irregular heartbeat
Slowed digestion causing pain, early fullness, nausea, bloating and constipation
Hepatitis of starvation, liver failure
Loss of period in females, low testosterone in males, infertility
Bone marrow suppression, anemia
Bone loss and osteoporosis
Thyroid abnormalities, low blood sugar
Brain atrophy, cognitive difficulty
Dry skin, hair loss, lanugo hair growth
Aspiration pneumonia, respiratory failure
High risk for refeeding syndrome, a potentially deadly complication of injudicious refeeding
Medical Complications of Bulimia Nervosa:
Dental erosion and infections, parotid gland swelling
Esophageal rupture
Gastroesophageal reflux (GERD), constipation
Low potassium, low sodium
Severe edema or fluid overload
Dehydration, fainting
Irregular heartbeat
Seizures
For Treatment:
First know the red flags. Red flags that may indicate an eating disorder include: Skipping meals
Making excuses for not eating
Eating only a few certain “safe” foods, usually those low in fat and calories
Adopting rigid meal or eating rituals, such as cutting food into tiny pieces or spitting food out after chewing
Cooking elaborate meals for others, but refusing to eat them themselves
Collecting recipes
Withdrawing from normal social activities
Persistent worry or complaining about being fat
A distorted body image, such as complaining about being fat despite being underweight
Not wanting to eat in public
Frequent checking in the mirror for perceived flaws
Wearing baggy or layered clothing
Repeatedly eating large amounts of sweet or high-fat foods
Use of syrup of ipecac, laxatives, the over-the-counter weight-loss drug orlistat (Alli), or over-the-counter drugs that can cause fluid loss, such as menstrual symptom relief medications
Use of dietary supplements or herbal products for weight loss
Food hoarding
Leaving during meals to use the toilet
Eating in secret
When to see a doctor
Because of its powerful pull, an eating disorder can be difficult to manage or overcome by yourself. Eating disorders can virtually take over your life. You may think about food all the time, spend hours agonizing over what to eat and exercise to exhaustion. You may feel ashamed, sad, hopeless, drained, irritable and anxious. You may also have a host of physical problems because of your eating disorder, such as irregular heartbeats, fatigue, and bowel or menstrual troubles. If you’re experiencing any of these problems, or if you think you may have an eating disorder, seek medical help.
Urging a loved one to seek treatment
Unfortunately, many people with eating disorders resist treatment. If you have a loved one you’re worried about, urge him or her to talk to a doctor. Even if your loved one isn’t ready to acknowledge having an issue with food, you may be able to open the door by expressing concern and a desire to listen. If you’re concerned your child may have an eating disorder, contact his or her doctor about your concerns. You can get a referral to qualified mental health providers for treatment.
Keep in mind, however, that in children it’s sometimes hard to tell what’s an eating disorder and what’s simply a whim, a new fad, or experimentation with a vegetarian diet or other eating styles. In addition, many girls and sometimes boys go on diets to lose weight, but stop dieting after a short time. If you’re a parent or guardian, be careful not to mistake occasional dieting with an eating disorder. On the other hand, be alert for eating patterns and beliefs that may signal unhealthy behavior, as well as peer pressure that may trigger eating disorders.
“Anorexia nervosa and bulimia nervosa are the most common clinically recognized eating disorders. Those with anorexia skip meals, adopt highly restrictive and unhealthy diets, obsess over thinness and food, and present abnormal eating habits or rituals.
Bulimia presents itself in the form of binging, or overeating, followed by purging, often either by vomiting or using laxatives.”
Diffen http://www.diffen.com
Anorexia Nervosa
Anorexia Nervosa is characterized by the refusal to eat. It can affect anyone of any gender or age but disproportionately affects young women in their late teens and early twenties.
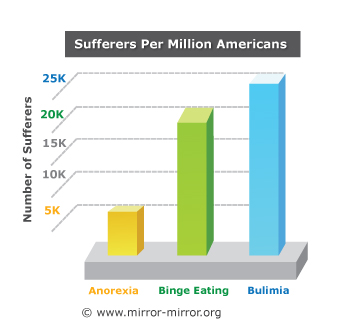
According to the most current edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) there are four diagnostic criteria that must be present to achieve having Anorexia Nervosa. First a person must refuse to maintain body weight over a minimal normal weight for age and height or have a failure to make expected weight gain during a defined period of growth, resulting in a body weight 15% lower than expected. Second, the person must experience intense fear of gaining weight or becoming fat, even though underweight. Third, the person must have a disturbance in the way his or her body weight, size, or shape is experienced and also experience undue influence of body weight, or shape on self-evaluation, or denial of the seriousness of the current body weight. Finally, amenorrhea must be present. Amenorrhe is the absence of at least three consecutive menstrual cycles when otherwise expected to occur. This eating disorder affects 0.4-percent of adolescents and young women. However it is estimated that more than 4-percent of all women will struggle with anorexia nervosa over the course of their lifetime.
Bulimia Nervosa
Bulimia Nervosa is characterized by cyclical bingeing and purging episodes. Bingeing is defined as the consumption of more food than most other people would eat in a similar circumstance over a discrete period of time accompanied by a sense of lack of control over the food consumption.
Bulimia Nervosa exists when bingeing and compensatory behaviors occur on average 2 times weekly or more for a period of at least 3 months, when the behaviors are not exclusively those of Anorexia Nervosa, and when self-evaluation is unduly influenced by body shape or weight. Those with Bulimia are often very concerned about gaining weight and intensely fear getting fat.
People with Bulimia may engage in a variety of either purging or non-purging behaviors such as vomiting, using laxatives, using diuretics, using enemas, fasting, or exercising excessively. Bulimic bingeing and purging cycles are often conducted in secret because of the shame and disgust associated with the process.
Bulimia nervosa is an eating disorder affects 1.3-percent of adolescents and young women. An additional 0.7-percent of older women will develop this disorder over the course of their life.
Learn tomorrow the other eating disorders. Eating Disorders is this week’s National Awareness Topic!
“Ablation is used to treat abnormal heart rhythms, or arrhythmias. The type of arrhythmia and the presence of other heart disease will determine whether ablation can be performed surgically or non-surgically.”
American Heart Association

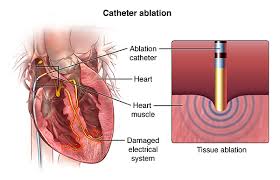
Ablation is used to treat abnormal heart rhythms, or arrhythmias. The type of arrhythmia and the presence of other heart disease will determine whether ablation can be performed surgically or non-surgically.
Ablation therapy using radio frequency waves on the heart is used to cure a variety of cardiac arrhythmiae such as supraventricular tachycardia, Wolff–Parkinson–White syndrome (WPW), ventricular tachycardia, and more recently as management of atrial fibrillation (especially when its newly diagnosed when medical management can’t change it back to normal sinus rhythm, which is the normal cardiac rhythm seen on a telemetry monitor or of an EKG taken on a patient).
An arrhythmia is a change in the heart’s normal rate or rhythm, normally between 60 and 100 beats per minute. Arrhythmias are classified by their location in the heart and by their speed or rhythm. An atrial arrhythmia is an abnormality that occurs in one of the two upper chambers of the heart, the left or right atrium. Arrhythmias are associated with aging and typically happen more frequently during middle age. At least 10 to 15 percent of people older than 70 years experience arrhythmias. We have what we call our human pacemaker of the heart that naturally sends conduction for the heart to pump, which is called the sinus node. This is in the upper left corner of the right chamber of the heart. That is where the name sinus rhythm derives from (the sinus node) which is the best rhythm a human can be in as long as the pulse rate stays above 60 and stays under 100. Now if that sinus node for some reason breaks down and no longer works; so than the pace site starts somewhere in the right atrium below the sinus node (the heart is compensating for whatever is the reason the sinus node is not working). So now the rhythms are called atrial rhythms because of where the new natural pacemaker site is in the heart. This is where ablation comes into play if the type of atrial rhythm they have is detrimental to the patient; including if that patient is a candidate for this procedure. Between our heart chambers on the top (called atriums) and below (called the ventricles) is a AV (meaning atrioventricular valve). Rhythms above the ventricles are also grouped as supraventricular rhythms. Which is what ablation is used for.
Types of rhythms a patient would be considered for ablation as a possible treatment:
Atrial fibrillation. The electrical signal that circles uncoordinated through the muscles of the atria (the upper chambers of the heart), causing them to quiver (sometimes more than 400 times per minute) without contracting. The ventricles (the lower chambers of the heart) do not receive regular impulses and contract out of rhythm, and the heartbeat becomes uncontrolled and irregular. It is the most common atrial arrhythmia, and 85 percent of people who experience it are older than 65 years.
Atrial fibrillation can cause a blood clot to form, which can enter the bloodstream and trigger a stroke. Underlying heart disease or hypertension increases the risk of stroke from atrial fibrillation as does age even without heart disease or hypertension.
Premature atrial contraction (PAC or premature atrial impulses). A common and benign arrhythmia, a PAC is a heartbeat that originates away from the sinus node, which sends electrical signals through the upper chamber. It typically occurs after the sinus node has initiated one heartbeat and before the next regular sinus discharge. A PAC can cause a feeling of a skipped heartbeat. Use of caffeine, tobacco, and/or alcohol, or stress can bring on PACs or increase their frequency.
Supraventricular tachycardia (SVT). Characterized by a rapid heart rate that ranges between 100 and 240 beats per minute, SVT usually begins and ends suddenly. SVT occurs when an electrical impulse ‘re-enters’ the atrial muscles. A disorder that a person may have at birth, SVT is commonly caused by a variation in the electrical system of the heart. SVT often begins in childhood or adolescence and can be triggered by exercise, alcohol, or caffeine. SVT is rarely dangerous, but can cause a drop in blood pressure, causing lightheadedness or near-fainting episodes, and, rarely, fainting episodes.
Atrial flutter. Differentiated from atrial fibrillation by its coordinated, regular pattern, atrial flutter is a coordinated rapid beating of the atria. Most who experience atrial flutter are 60 years and older and have some heart disorder, such as heart valve problems or a thickening of the heart muscle. Atrial flutter is classified into two types, according to the pathways responsible for it. Type I normally causes the heart rate to increase to and remain at 150 beats per minute. Rarely, the rate may reach 300 beats per minute; sometimes it decreases to 75 beats per minute. Type II increases the atrial rate faster, so the ventricular rate may be 160 to 170 beats per minute. As with atrial fibrillation, atrial flutter increases the risk of stroke.
Sick sinus syndrome (SSS). Common among older people, SSS is an improper firing of electrical impulses caused by disease or scarring in the sinus or Sinoatrial node (SA node). SSS normally causes the heart rate to slow, but sometimes it alternates between abnormally slow and fast. A progressive condition, with episodes increasing in frequency and duration, SSS can be caused by:
Sinus tachycardia. The sinus node emits abnormally fast electrical signals, which increases the heart rate to between 100 beats per minute to 140 beats per minute at rest, and 200 beats per minute during exercise. A normal response to exercise or stress, it can also be caused by:
Sinus bradycardia. Associated with impaired impulse generation in the SA node, it causes the heart rate to decrease to fewer than 60 beats per minute. Commonly caused by SSS, drugs like beta-blockers and calcium-channel blockers can also cause sinus bradycardia. Occasionally sinus bradycardia can be caused by impaired conduction of impulses to the atrial muscles.
Wolff-Parkinson-White syndrome (WPW). WPW syndrome occurs when electrical signals fail to pause in the atrioventricular node because an extra pathway allows the impulse to “bypass” the normal pathway; and the syndrome is sometimes called bypass tract. WPW syndrome causes heart rates approaching 240 beats per minute.
Occasionally, impulses can go down one extra pathway and up another, creating a “loop” or “short circuit,” (called SVT because of WPW). Patients with WPW syndrome may develop atrial fibrillation and are at increased risk for developing a dangerous ventricular arrhythmia when this occurs.
CAUSES AND RISK FACTORS
Problems with the heart’s electrical system or with the muscles’ response to the signal can cause arrhythmias. Physicians have categorized arrhythmias to their type:
People without heart disease can develop an arrhythmia for unknown causes, but risk factors can include:
WHAT ARE THE SYMPTOMS?
|
|
The onset and duration of arrhythmia symptoms vary according to its type, frequency, duration, and whether structural heart disease is present.
Common symptoms that people experience may include:
Certain arrhythmias may cause fainting, and, occasionally stroke, while others (‘silent’ arrhythmias) cause no symptoms.
DIAGNOSIS
Arrhythmias can be difficult to diagnose because they can be unpredictable and brief. A physician will typically take a person’s medical history, and perform a physical examination, during which the physician may detect an arrhythmia using a stethoscope. Arrhythmias that occur infrequently, last for short periods of time, or do not cause noticeable symptoms may require more detailed tests, such as:
“Acne is the most common skin condition in the United States. Although it’s common, accurate information about acne can be scarce.”
American Academy of Dermatology
“Diabetes Mellitus (DM) is a complex chronic disease involving disorders in carbohydrate, protein, and fat metabolism and the development of macro-vascular, micro-vascular, neurological complications that don’t occur over a few nights or weeks or months.”
American Diabetes Association