Stage II colorectal cancer is divided into three subcategories: IIA, IIB and IIC.
The difference between the categories lies in the extent to which the cancer has spread.
- Stage IIA (T3, N0, M0): The cancer has grown into the outermost layers of the colon or rectum, but has not grown through them. It has not reached nearby organs or lymph nodes, and has not spread to distant organs.
- Stage IIB (T4a, N0, M0): The cancer has grown through all of the layers of the colon or rectum, but has not grown into other organs or tissues.
- Stage IIC (T4b, N0, M0): The cancer has grown through all of the layers of the colon or rectum, and has grown into nearby organs or tissues. The cancer has not spread to the lymph nodes Surgery
- Initial treatment for stage II colon cancer is surgery to remove the section of colon that contains the tumor and surrounding tissue with its blood vessels and lymph nodes.
- The most commonly recommended protocols for patients diagnosed with stage II colon cancer:
Colectomy
A colectomy (or colon resection) is abdominal surgery that removes the section of colon where the tumor is located, tissue containing blood and lymph vessels surrounding the colon (mesentery), healthy tissue margins on either side and, if possible, at least 12 lymph nodes. Then the remaining ends of colon are reconnected with sutures or staples. This connection is called an anastomosis.
There are two types of surgery:
- Open colectomy: An incision is made in the abdomen, surgery performed through the opening, and the incision closed with sutures and/or staples.
- Laparoscopic colectomy: Three small keyhole incisions are made in the abdomen to insert a lighted instrument and specially designed surgical instruments that can be manipulated within the abdomen. Sometimes an incision is made just long enough for the surgeon’s hand to assist during laparoscopy. This is also known as minimally invasive surgery.If your lymph nodes are cancer-free (also known as node-negative), your diagnosis is stage II colon cancer
- The tumor, tissue on either side of it (the margins), and fat and lymph nodes attached to the colon are removed for further study by a pathologist. The pathologist evaluates the cancer cells in the tumor itself, looks for cancer in the margins and other tissue, and studies as many lymph nodes as possible in order to provide an accurate diagnosis.
Chemotherapy
Treatment of node-negative stage II colon cancer is controversial. While surgery to remove the tumor in the colon is universally accepted as initial treatment, the value of chemotherapy after that surgery to keep cancer from recurring (coming back) is hard for patients and doctors to judge.
It’s estimated that between four and five percent of patients with stage II colon cancer will benefit from chemotherapy. However, there are also side effects, some severe, associated with chemotherapy. Very few patients will die as a result of chemotherapy.
Because of the risks of treatment, researchers are looking for ways to identify patients who are at higher risk for recurrence, who are most likely to benefit from chemotherapy.
Some factors have been identified that lead to higher risk for stage II patients including:
- T4 tumors that extend beyond the outer wall of the colon into adjacent tissues and organs
- Too few lymph nodes removed and examined (less than 12)
- Cancer cells in blood and lymph vessels surrounding the tumor (not the same as lymph nodes)
- Undifferentiated or poorly differentiated tumors
- Perforation (a hole) of the colon by the tumor
- A tumor that obstructs (closes off) the colonFor high-risk stage II patients, the number needed to prevent one recurrence or death is smaller, probably 15 to 30 patients.
- It may help your decision to think about the problem in terms of numbers: In order to prevent one recurrence or death from all cases of stage II colon cancer, 25 to 50 patients need to receive chemotherapy. One in six of those patients will have a severe side effect; one in 100 to 200 will die as a result of treatment.
Chemotherapy regimens for high-risk stage II colon cancer:
- FOLFOX: combination treatment with infusional 5-FU (fluorouracil), leucovorin, and oxaliplatin
- FLOX: combination with bolus 5-FU, leucovorin, and oxaliplatin (severe diarrhea is more common with FLOX than FOLFOX but outcomes are similar)
- Xeloda (capecitabine): oral “prodrug” which is converted to 5-FU in the tumor
- 5-FU and leucovorinThere are some indicators of a patient’s risk of recurrence of their cancer, but no clear information that higher risk means they may benefit from therapy — thus there are research efforts underway to better define “risk” and develop treatments that will benefit the higher risk patient in a predictable way.
- Stage III colorectal cancer treatments:In this article
- Your doctor can discuss the advantages and disadvantages of the different chemotherapy regimens if you decide to proceed with chemotherapy after your surgery. Chemotherapy usually lasts about six months.
Stage III Colorectal Cancer Treatments
Stage III colorectal cancers have spread outside the colon to one or more lymph nodes (small structures that are found throughout the body that produce and store cells that fight infection). Tumors within the colon wall, which also involve the lymph nodes are classified as stage IIIA, while tumors that have grown through the colon wall and have spread to one to four lymph nodes are classified as stage IIIB cancers. Those tumors, which have spread to more than four lymph nodes are classified as stage IIIC colon cancers.
Treatment involves:
- Surgery to remove the tumor and all involved lymph nodes if possible.
- After surgery, the patient will receive chemotherapy with 5-FU, leucovorin and oxaliplatin, capecitabine with oxaliplatin or capecitabine alone.
- Radiation may be needed if the tumor is large and invading the tissue surrounding the colon.
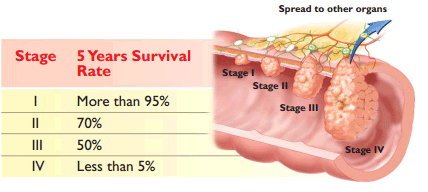
The five-year survival rate for stage III colon cancer is about 64%. Patients with one to four positive lymph nodes have a higher survival rate than people with more than five positive lymph nodes.
Stage IV Colorectal cancer treatments:
Stage IV colorectal cancers have spread outside the colon to other parts of the body, such as the liver or the lungs. Cancer that has spread is also called “metastatic.” The tumor can be any size and may or may not include affected lymph nodes (small structures that are found throughout the body that produce and store cells that fight infection).
Treatment may include:
- Removal of the cancer surgically or another surgical procedure to bypass the colon cancer and hook up healthy colon (an anastomosis).
- Surgery to remove parts of other organs such as the liver, lungs, and ovaries, where the cancer may have spread.
- Chemotherapy to relieve symptoms and improve survival.
- Erbitux, Avastin, or Vectibix in combination with standard chemotherapy, depending upon tumor characteristics.
- Zaltrap is a drug also approved for use with chemotherapy in cases where the cancer has progressed or is resistant to treatment.
- Stivarga is a targeted therapy approved in patients whose cancer has progressed after previous therapy.
- Clinical trials of new chemotherapy regimens, or immunological therapy.
- Radiation to relieve symptoms.
The five-year survival rate for stage IV colon cancer is nearly 8% or less.