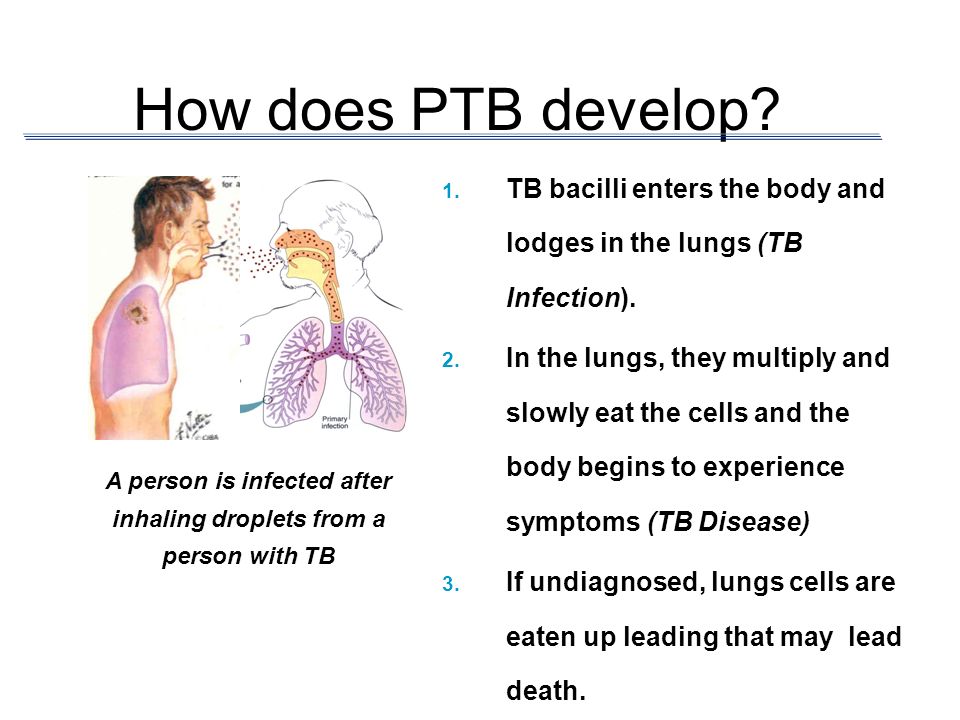
How does PTB develop? TB bacilli enters the body and lodges in the lungs (TB Infection). In the lungs, they multiply and slowly eat the cells and the body begins to experience symptoms (TB Disease) A person who develops a TB disease, when remain untreated, can then begin to infect others. In some cases, the TB germ migrates to other body organs and begin to destroy them, thus the advent of extra-pulmonary (outside) cases of Tuberculosis like TB of the meninges, bones, etc. A TB disease that remains untreated leads to death.
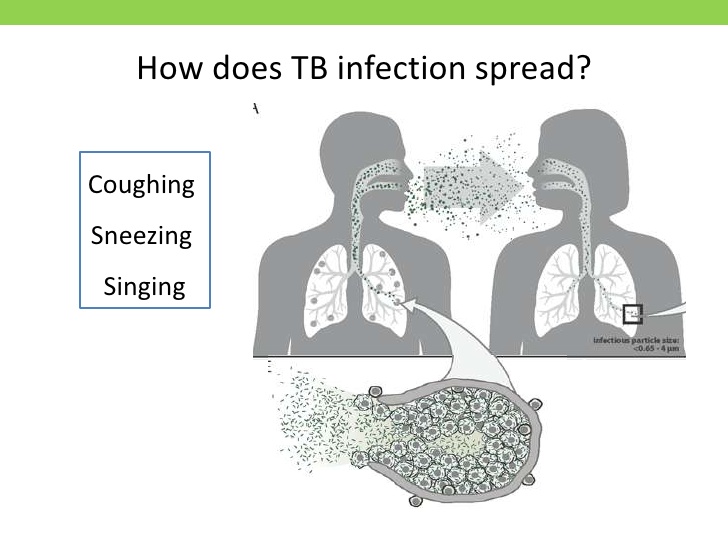
Airborne to prevent the transmission of highly contagious or virulent infections spread by small airborne droplets (smaller than 5 microns) examples know or suspected TB, chicken pox.
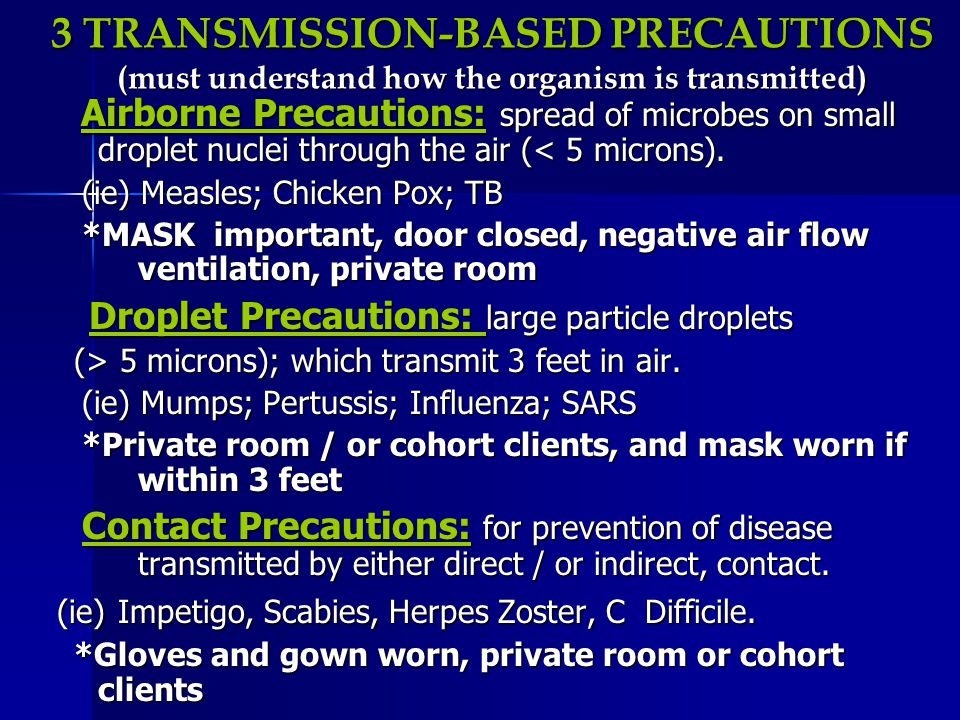
Airborne Precautions: spread of microbes on small droplet nuclei through the air ( 5 microns); which transmit 3 feet in air. (ie) TB, Mumps; Pertussis; Influenza; SARS. Private room / or cohort clients, and mask worn if within 3 feet.
TB can be transmitted in just about any setting. It can be spread in places such as homes or worksites. However, TB is most likely to be transmitted in health care settings when health care workers and patients come in contact with persons who have unsuspected TB disease, who are not receiving adequate treatment, and who have not been isolated from others. All health-care settings need an infection-control program designed to ensure the following:
- Prompt detection of TB disease;
- Airborne precautions; and
- Treatment of people who have suspected or confirmed tuberculosis (TB) disease.
Overview of TB Infection-Control Measures
The TB infection-control program should be based on the following three-level hierarchy of control measures:
- Administrative controls
- Environmental controls
- Use of respiratory protective equipment
Administrative Controls
The first and most important level of the hierarchy, administrative controls, are management measures that are intended to reduce the risk or exposure to persons with infectious TB. These control measures consist of the following activities:
- Assigning someone the responsibility for TB infection control in the health care setting;
- Conducting a TB risk assessment of the setting;
- Developing and implementing a written TB infection-control plan;
- Ensuring the availability of recommended laboratory processing, testing, and reporting of results;
- Implementing effective work practices for managing patients who may have TB disease;
- Ensuring proper cleaning, sterilization, or disinfection of equipment that might be contaminated (e.g., endoscopes);
- Educating, training, and counseling health care workers, patients, and visitors about TB infection and disease;
- Testing and evaluating workers who are at risk for exposure to TB disease;
- Applying epidemiology-based prevention principles, including the use of setting-related TB infection-control data;
- Using posters and signs to remind patients and staff of proper cough etiquette (covering mouth when coughing) and respiratory hygiene; and
- Coordinating efforts between local or state health departments and high-risk health-care and congregate settings.
Environmental Controls
The second level of the hierarchy is the use of environmental controls to prevent the spread and reduce the concentration of infectious droplet nuclei. This includes two types of environmental control.
- Primary environmental controls consist of controlling the source of infection by using local exhaust ventilation (e.g., hoods, tents, or booths) and diluting and removing contaminated air by using general ventilation.
- Secondary environmental controls consist of controlling the airflow to prevent contamination of air in areas adjacent to the source airborne infection isolation (AII) rooms; and cleaning the air by using high efficiency particulate air (HEPA) filtration, or ultraviolet germicidal irradiation.
Respiratory Controls
The third level of the hierarchy is the use of respiratory-protection control. It consists of the use of personal protective equipment in situations that pose a high risk of exposure to TB disease.
Use of respiratory protection equipment can further reduce risk for exposure of health care workers to infectious droplet nuclei that have been expelled into the air from a patient with infectious TB disease. The following measures can be taken to reduce the risk for exposure:
- Implementing a respiratory protection program;
- Training health care workers on respiratory protection; and
- Educating patients on respiratory hygiene and the importance of cough etiquette procedures.
Determining the Infectiousness of TB Patients
The infectiousness of a TB patient is directly related to the number of droplet nuclei carrying M. tuberculosis (tubercle bacilli) that are expelled into the air. The number of tubercle bacilli expelled by a TB patient depends on the following factors:
- Presence of a cough
- Cavity in the lung
- Acid-fast bacilli on sputum smear
- TB disease of the lungs, airway, or larynx
- Patient not covering mouth and nose when coughing
- Not receiving adequate treatment or having prolonged illness
- Undergoing cough-inducing procedures
- Positive sputum cultures
Patients can be considered noninfectious when they meet all of the following three criteria:
- They have three consecutive negative AFB sputum smears collected in 8- to 24-hour intervals (one should be an early morning specimen);
- They are compliant with an adequate treatment regimen for two weeks or longer; and
- Their symptoms have improved clinically (for example, they are coughing less and they no longer have a fever).