“I’m not a big drinking person and hardly ever have alcohol. Perhaps it’s not sweet enough for my sweet tooth.”
Dawn French (born 11 October 1957 – is an English actress, writer, and comedian)
“I’m not a big drinking person and hardly ever have alcohol. Perhaps it’s not sweet enough for my sweet tooth.”
Dawn French (born 11 October 1957 – is an English actress, writer, and comedian)
 But than we are stuck with the 80% Nonfunctional hurting society, not worth it!
But than we are stuck with the 80% Nonfunctional hurting society, not worth it!

Alcoholism, or alcohol dependence, is a disease that causes
With alcohol abuse, you are not physically dependent, but you still have a serious problem. The drinking may cause problems at home, work, or school. It may cause you to put yourself in dangerous situations, or lead to legal or social problems.
Alcohol use disorder (which includes a level that’s sometimes called alcoholism) is a pattern of alcohol use that involves problems controlling your drinking, being preoccupied with alcohol, continuing to use alcohol even when it causes problems, having to drink more to get the same effect, or having withdrawal symptoms when you rapidly decrease or stop drinking.Unhealthy alcohol use includes any alcohol use that puts your health or safety at risk or causes other alcohol-related problems. It also includes binge drinking — a pattern of drinking where a male consumes five or more drinks within two hours or a female downs at least four drinks within two hours. Binge drinking causes significant health and safety risks. If your pattern of drinking results in repeated significant distress and problems functioning in your daily life, you likely have alcohol use disorder. It can range from mild to severe. However, even a mild disorder can escalate and lead to serious problems, so early treatment is important.
Another common problem is binge drinking. It is drinking about five or more drinks in two hours for men. For women, it is about four or more drinks in two hours.
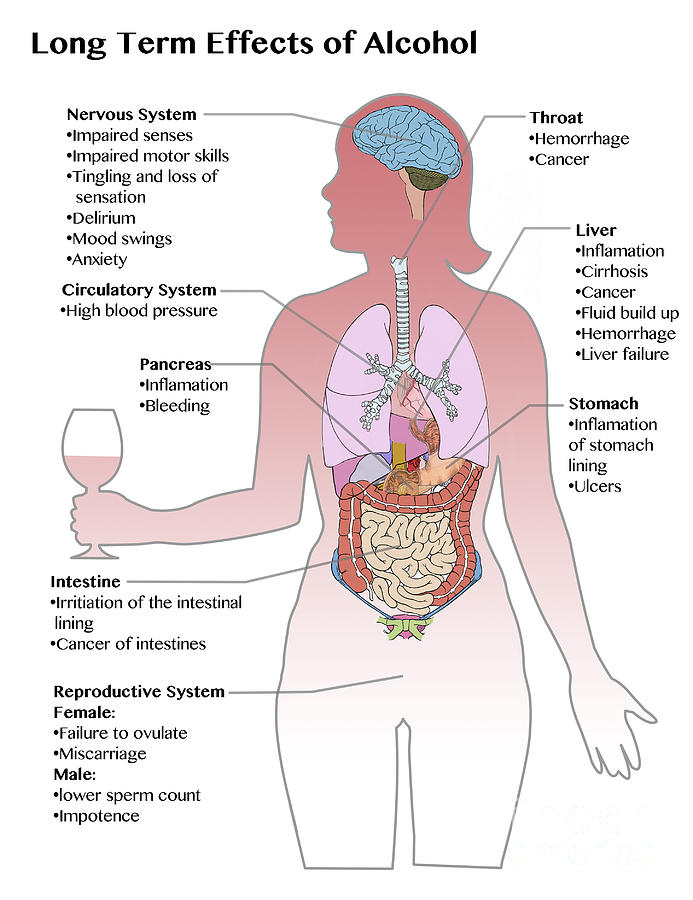
Too much alcohol is dangerous. Heavy drinking can increase the risk of certain cancers. It can cause damage to the liver, brain, and other organs. Drinking during pregnancy can harm your baby. Alcohol also increases the risk of death from car crashes, injuries, homicide, and suicide.
**Genetic, psychological, social and environmental factors can impact how drinking alcohol affects your body and behavior. Theories suggest that for certain people drinking has a different and stronger impact that can lead to alcohol use disorder.
Over time, drinking too much alcohol may change the normal function of the areas of your brain associated with the experience of pleasure, judgment and the ability to exercise control over your behavior. This may result in craving alcohol to try to restore good feelings or reduce negative ones.**
Alcohol use disorder can include periods of alcohol intoxication and symptoms of withdrawal.
Alcohol use disorder can be mild, moderate or severe, based on the number of symptoms you experience. Signs and symptoms may include:

Epilepsy
Most people with epilepsy are otherwise healthy; as long as it is controlled like most other diseases. A seizure is a physical manifestation of paroxysmal and abnormal electrical firing of neurons in the brain. Think of it as numerous voltage (hyperexcitability of neurons) going throughout the brain meaning brain waves going in all directions with the brain saying its too much activity causing the brain to go into a seizure.
When the seizure occurs there is a decrease in oxygen since the brain isn’t capable to send messages during the seizure. If the seizure continues to repeat one right after another the person is in status epilepticus and if the seizures doesn’t stop the person can lead to a neuronal death; like John Travolta’s son who died of this.
The term seizure disorder may refer to any number of conditions that result in such a paroxysmal electrical discharge. These conditons could be metabolic or structural in nature. Epilepsy is the term for those who have a second seizure that occurs spontaneously and without preceding metabolic or structural cause for the occurrence. Epilepsy is a chronic disorder that requires antiepileptic drug therapy; usually thorough out life.
Etiology of Epilepsy is generally a sign of underlying pathology involving the brain. It may be the first sign of nervous system disease (ex. Brain tumor), or it may be a sign of a systemic or metabolic derangement.
Metabolic and Systemic Causes of Seizures:
a.) Electrolyte Imbalance=Acidosis, heavy metal poisoning, Hypocalcemia, Hypocapnea, Hypoglycemia, Hypoxia, Sodium-Potassium imbalance, Systemic diseases (liver, renal failure, etc…) Toxemia of pregnancy, and water intoxication.
b.) Infections like meningitis, encephalitis, brain abcess.
c.) Withdrawal of sedative-hypnotic drugs=Alcohol, Antiepileptic drugs, Barbiturates, Benzodiazepines.
d.) Iatrogenic drug overdose=Theopylline, Penicillin.
Other causes of epilepsy can be Trauma, Heredity.
Structural causes of epilepsy:
Head trauma/Degenerative Disease like Alzheimer’s or Creutfeldz-Jacob or Huntington’s Chorea or Multiple Sclerosis or Pick’s Disease. There is also tumors or genetic disease or Stroke or Infections or Febrile seizures.
Types of seizures
I-Partial seizures (seizures beginning local)
1-simple partial seizures-(the person is conscious and not impaired). With motor symptoms, autonomic symptoms and even psychic symptoms.
2.)-Complex partial seizures-(the person is with impairment of consciousness)
II-Generalized seizures-(bilaterally symmetrical and without local onset).
3.) Tonic clonic seizures – Grand Mal
Diagnosis
The history of the person is the most valuable component of the workup of that individual with possible epilepsy.
The routine diagnostic tooling to see if someone has this disease is a EEG which is the major diagnostic test. EEG takes short samples of brain wave activity with 26 wires to the scalp recording amplified brain waves from the superficial regions of the brain by means of scalp electrodes.
Laboratory studies are done to rule out various causes for seizures. Routine blood and urine studies are often done for baseline information. Electrolytes and blood chemistries will be evaluated to identify possible metabolic causes for seizures.
Neuropsychological testing may be done in the evaluation of persons presenting with seizures. The purpose of neuropsychological testing is to determine if there is brain dysfunction and to determine if the pattern of change in brain function is indicative of a destructive lesion. Neuropsychological testing involves evaluation of cognitive functions and personality and emotional traits.
Medical Management
The major medical treatment for epilepsy is antiepileptic medications. Epileptic seizures can be controlled in 50 to 95% of cases with this form of treatment depending on seizure type and compliance of the individual taking their medications.
Those taking medications for epilepsy know if a single first line drug is not effective a second first lin drug is added but the noneffective drug is tapered off while the second first line drug is given. Know during this time frame there is a risk for seizure activity so practice safety (ex. do not drive).
In some cases there is surgery: those with intractable seizures is the epileptic focus may be possible. In some cases partial complex seizures are the common seizure treated by surgery. The focus of this seizure type has often been found in the anterior temporal and inferior frontal regions of the brain cortex.
There are other treatments as well.
Care during a Seizure what do we do and what is the major concerns for the individual seizing:
The care of a person in a seizure should focus primarily on maintaining a safe environment. The seizure that has greatest risk for causing injury and even fatality is the generalized tonic/clonic (grand mal), although there is a potential for injury with any seizure that involves alteration of consciousness.
The 2 major goals for care during a seizure are protection from injury and prevention of aspiration. The person’s head should be cradled if on the floor to prevent banging of the head. At no time should the person be restraint when having a seizure. The person should be turned to their side to allow the tongue to fall away from the airway and allow drainage of the excessive saliva that accumulates to drain out of the mouth during the seizure. You should stay with the person till the seizure stops and note the behavior mentally and physically the person exhibits while having the seizure and how long it lasts. Immediately call 911 (especially if this is the first seizure the person ever had) or call the neurologist of the individual to have the him or her be evaluated ASAP.
“The body cannot produce enzymes in perfect combinations to metabolize your foods as completely as the food enzymes created by nature do. This results in partially digested fats, proteins, and starches that can clog your body’s intestinal tract and arteries.”
Charlie Trotter (September 8, 1959 – November 5, 2013) was an American chef and restaurateur.
“When I work, a lot of times I have to lose weight, and I do that, but in my regular life I was not eating right, and I was not getting enough exercise. But by the nature of my diet and that lifestyle – boom! The end result was high blood sugars that reach the levels where it becomes Type 2 diabetes. I share that with a gajillion other people.”
Tom Hanks (actor)
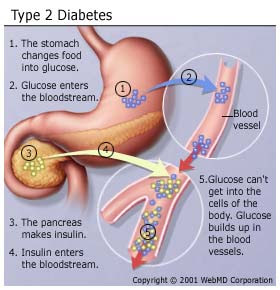
Diabetes Mellitus (DM) is a complex chronic disease involving disorders in carbohydrate, protein, and fat metabolism and the development of macro-vascular, micro-vascular, neurological complications that don’t occur over a few nights or weeks or months. It is a metabolic disorder in where the pancreas organ ends up causing many disruptions in proper working of our body. The pancreas is both an endocrine and exocrine gland. The problem with diabetes is due to the endocrine part of the pancreas not working properly. More than 1 million islet cells are located throughout the organ. The three types of endocrine cells that the pancreas excretes into our blood stream are alpha, beta, and delta cells. The alpha cells secrete glucagon (stored glucose), beta secrete insulin, and delta secrete gastrin and pancreatic somatostatin. A person with DM has minimal or no beta cells secreted from the pancreas, which shows minimal or no insulin excreted in the person’s bloodstream. Insulin is necessary for the transport of glucose, amino acids, potassium, and phosphate across the cell membrane getting these chemical elements into the cell. When getting these elements into the cells it is like the cell eating a meal and the glucose, being one of the ingredients in the meal, is used for energy=fuel to our body; the glucose inside the cells gets carried to all our tissues in the body to allow the glucose to be utilized into all our tissues so they can do their functions (Ex. Getting glucose into the muscle tissue allows the muscles to have the energy to do the range of motion in letting us do our daily activities of living, like as simple as type or walk). The problem with diabetes is the glucose doesn’t have the insulin being sent into the bloodstream by the pancreas to transfer the glucose across the cell membrane to be distributed as just discussed. Instead what results is a high glucose levels in the blood stream causing hyperglycemia. It should be apparent that when there is a deficit of insulin, as in DM, hyperglycemia with increased fat metabolism and decreased protein synthesis occur ( Our body being exposed to this type of environment over years causes the development of many chronic conditions that would not have occurred if DM never took place in the body, all due to high glucose levels starting with not being properly displaced in the body as it should be normally.).
People with normal metabolism upon awaking and before breakfast are able to maintain blood glucose levels in the AM ranging from 60 to 110mg/dl. After eating food the non-diabetic’s blood glucose may rise to 120-140 mg/dl after eating (postprandial), but these then rapidly return back to normal. The reason for this happening is you eat food, it reaches the stomach, digestion takes place during digestion the stomach brakes down fats, carbohydrates, and sugars from compound sugars to simple sugars (fructose and glucose). Than the sugars transfer from the stomach into the bloodstream causing an increase in sugar levels. Now, your body uses the sugar it needs at that time throughout the entire body for energy and if still extra sugar left in the bloodstream that isn’t needed at that time to be utilized it now needs to go somewhere out of the bloodstream to allow the glucose blood level to get back between 60-110mg/dl. That extra glucose first gets stored up in the liver 60-80% and then gets stored in our fat tissue=fat storage=weight increase. Unfortunately this doesn’t take place with a diabetic since there is very little or no insulin being released by the pancreas and over time due to the high blood glucose blood levels (called hyperglycemia) problems arise in the body over years. When diabetes occurs there is a resolution and you have the disease the rest of your life. You need to control your glucoselevel.
2 TYPES OF DM: a.)Diabetes I & b.) Diabetes ll. We have risk factors that can cause disease/illness; there are unmodified and modified risk factors.
With unmodified risk factors we have no control in them, which are 4 and these are:
1-Heredity 2-Sex 3-Age 4-Race.
Now modified risk factors are factors we can control, 3 of them that you can control:
They are 1.)your weight 2.)diet 3.)health habits (they play a big role for many people getting DM II).
Look at what the Mayo Clinic (www.mayoclinic.com /health/diabetes)says about risk factors:
RISK FACTOR FOR TYPE DIABETES ONE:
Although the exact cause of type 1 diabetes is unknown, genetic factors can play a role. Your risk of developing type 1 diabetes increases if you have a parent or sibling who has type 1 diabetes. Based on research, we also know that genes account for less than half the risk of developing type1 disease. These findings suggest that there are other factors besides genes that influence the development of diabetes. We don’t know what these factors are, but a number of different theories exist. Environmental factors, such as exposure to a viral illness, also likely play some role in type 1 diabetes. Other factors that may increase your risk include:
The presence of damaging immune system cells that make autoantibodies. Sometimes family members of people with type 1 diabetes are tested for the presence of diabetes autoantibodies. If you have these autoantibodies, you have an increased risk of developing type 1 diabetes. But, not everyone who has these autoantibodies develops type 1.
Dietary factors. A number of dietary factors have been linked to an increased risk of type 1 diabetes, such as low vitamin D consumption; early exposure to cow’s milk or cow’s milk formula; or exposure to cereals before 4 months of age.
Race. Type 1 diabetes is more common in whites than in other races.
Geography. Certain countries, such as Finland and Sweden, have higher rates of type 1 diabetes.
RISK FACTORS FOR DIABETES TYPE 2 AND PREDIABETES Researchers don’t fully understand why some people develop prediabetes and type 2 diabetes and others don’t. It’s clear that certain factors increase the risk, however, including:
Weight. The more fatty tissue you have, the more resistant your cells become to insulin.
Inactivity. The less active you are, the greater your risk. Physical activity helps you control your weight, uses up glucose as energy and makes your cells more sensitive to insulin. Exercising less than three times a week may increase your risk of type 2 diabetes.
Family history. Your risk increases if a parent or sibling has type 2 diabetes.
Race. Although it’s unclear why, people of certain races — including blacks, Hispanics, American Indians and Asians — are at higher risk.
Age. Your risk increases as you get older. This may be because you tend to exercise less, lose muscle mass and gain weight as you age. But type 2 diabetes is also increasing dramatically among children, adolescents and younger adults.
Gestational diabetes. If you developed gestational diabetes when you were pregnant, your risk of developing prediabetes and type 2 diabetes later increases. If you gave birth to a baby weighing more than 9 pounds (4 kilograms), you’re also at risk of type 2 diabetes.
Polycystic ovary syndrome. For women, having polycystic ovary syndrome — a common condition characterized by irregular menstrual periods, excess hair growth and obesity — increases the risk of diabetes.
High blood pressure. Having blood pressure over 140/90mm Hg is linked to an increased risk of type 2 diabetes.
Abnormal cholesterol levels. If you have low levels of high-density lipoprotein (HDL), or “good,” cholesterol, your risk of type 2 diabetes is higher. Low levels of HDL are defined as below 35 mg/dL.
High levels of triglycerides. Triglycerides are a fat carried in the blood. If your triglyceride levels are above 250 mg/dL, your risk of diabetes increases.
RISK FACTORS FOR GESTATIONAL DIABETES
Any pregnant woman can develop gestational diabetes, but some women are at greater risk than are others. Risk factors for gestational diabetes include:
Age. Women older than age 25 are at increased risk.
Family or personal history. Your risk increases if you have prediabetes — a precursor to type 2 diabetes — or if a close family member, such as a parent or sibling, has type 2 diabetes. You’re also at greater risk if you had gestational diabetes during a previous pregnancy, if you delivered a very large baby or if you had an unexplained stillbirth.
Weight. Being overweight before pregnancy increases your risk.
Race. For reasons that aren’t clear, women who are black, Hispanic, American Indian or Asian are more likely to develop gestational diabetes.
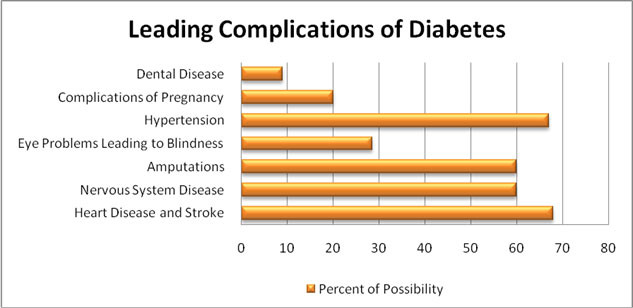
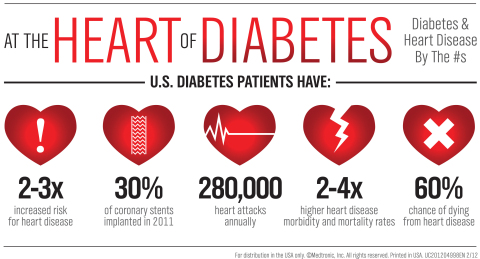
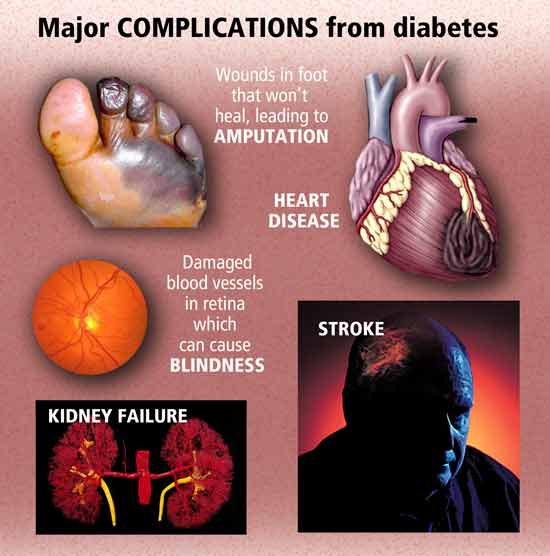
The key not to get diabetes is taking Prevention Measures (especially regarding type II) but even diagnosed with diabetes there are measures you can take in helping to control the glucose and decreasing the chances of increasing the side effects of what it can cause to the human body organs overtime especially cardiac disease, kidney disease, neuropathy, retinopathy to blind from having hyperglycemia frequently over years; in time it thickens the blood making circulation difficulty effecting tissues furthest from the heart= feet/lower extremities where skin ulcers occur for not getting enough oxygen to the tissues in the feet or lower extremities that can lead to necrosis causing amputation of toes to foot to below knee amputation to even above knee amputation. It also increases chance of heart attack and stroke. PREVENTION first and CONTROL second when diagnosed with DM, is so vitally important.
So help control your diabetes through diet (eating a low glucose or sugar diet=1800 to 2000 calories a day as your m.d. prescribes for you), weight (get in therapeutic weight range), and practice healthy habits. My blog can help guide you those in wanting to prevent diabetes by helping you lose weight by eating 6 low glycemic meals a day which allows low fat, low carbohydrates, low sugar keeping your baseline glucose at a steady level and low sugar level more on a regular basis with still treating yourself to occasional high glycemic meals when you’re in ideal weight. Follow this plan and in the first week eating like this I lost 5lbs or more and in the second week another 5lbs and since 1 to 2 lbs. per week . If you don’t, you put your diet 3 days back. This would definitely benefit you in prevention but if not or if diagnosed with diabetes always check with your doctor regarding diet, activity, and new health habits you may start, especially through this diet and make the alterations you need to do as your m.d. recommends. Recommended is have your m.d. give you clearance to start any new program if diagnosed with DM. I lost 22lbs already and I’m not obese by the body mass index. When I made this a routine in my life it got so EASY since I put health before my taste buds desires. It took time for not cheating with the food but it worked.
“People have known for centuries that certain foods can be good for your eyesight, including 16th Century Spanish explorers who carried chili peppers on voyages to help with night vision. Your mom and the explorers were smart: those chili peppers contained beta-carotene, vitamins C, E and B6, and folic acid, and the carrots had carotenoids and antioxidants. A diet rich in these nutrients may reduce the risk of developing macular degeneration and slow the prog…ression of the disease in those already diagnosed.”
NIH National Eye Institute