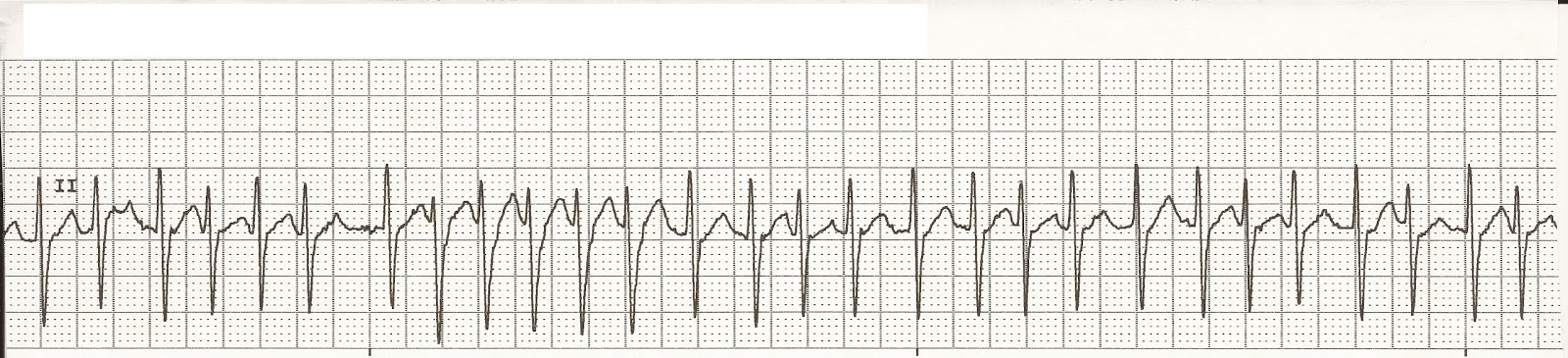
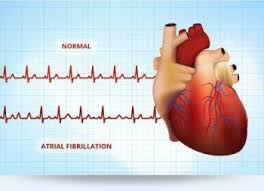
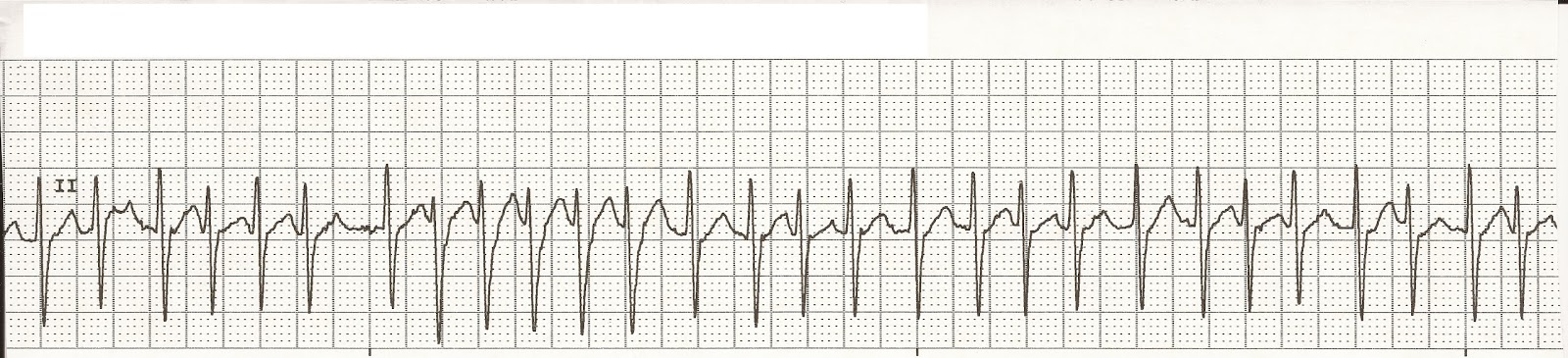
Top Line is Controlled AFIB less than 100 bts/min. Look how many spikes there are on the top line that’s the HR/min 8spikes x 10=80 in a 6 second strip from a EKG machine. Controlled afib is your HR under 100/min.
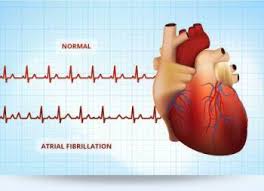
Bottom Line is Normal ( Sinus) rhythm, see how evenly spaced the spikes are. The rhythm rate is 5 spikes x 10=50 or a pulse or HR in a 6 second strip from a EKG machine. It’s not irregular and no stress to the heart.
A regular HR allows the heart chambers to fill up properly as opposed to irregular. This allows less stress on the heart. Ex an engine running properly in our car as opposed to not running properly puts a high potential for the engine to go into problems. Same with an irregular HR for the heart.
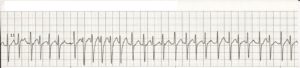
Each spike represents a heart pulsation which is when the organ is going lub dub, when the heart is contracting then relaxing, add them up on each strip on a 6 second strip (those above) x 10 tells you the heart rate by counting the spikes than x 10=that person’s heart rate. The first strip above is only 80 of a heart rate in 60 seconds and the next one is in RVR=280 of a HR. The heart can only take that so long before going into a worse rhythm called V-Tac or Ventricular Fibrillation and have to be shocked. So it is vital to keep atrial fibrillation under control meaning pulse under 100 beats a minute. Remember in a-fib. your upper chambers are in fibrillation (just quivering) as opposed to ventricular fibrillation, which is when we shock a pt. to knock their rhythm back to a better rhythm to stay alive. In Vent.Fib. untreated results into death since the chambers are doing nothing but quivering. The brain can live only 7 seconds without oxygen and barely any 02 is getting to your tissues in this rhythm.

 The heart is our ENGINE!
The heart is our ENGINE!
Some people in the US have this cardiac condition called Atrial Fibrillation where some with this condition even experience Rapid Ventricular Rate or Response with it.
Atrial fibrillation is an irregular and often rapid heart rate that commonly causes poor blood flow to the body.
During atrial fibrillation, the heart’s two upper chambers (the atria) beat chaotically and irregularly — out of coordination with the two lower chambers (the ventricles) of the heart causing your pulse to be irregular. We know now how the blood flows through the heart but due to the irregularity of the atriums which is not allowing the chambers to fill up to the maximal level they normally did when they didn’t have Atrial Fibrillation is decreasing the cardiac output (blood volume) from the left ventricle to be decreased. This means the heart and all other tissus aren’t getting the regular amount of oxygen they got when they were in a regular normal rhythm. Atrial fibrillation symptoms often include heart palpitations, shortness of breath and weakness. Atrial fibrillation (also called AFib or AF) is a quivering or irregular heartbeat (arrhythmia) that can lead to blood clots, stroke, heart failure and other heart-related complications. Some people refer to AFib as a quivering heart. What happens here is primarily the ventricles take over. With the atriums quivering and the ventricles going at their rate this causes an irregular heart rate=HR. Another problem with an irregular heart rate is this allows blood to pool in the heart putting the patient at risk for clot formation. As this HR gets more irregular it puts the patient at a higher risk of allowing the clot to break off inside the heart now flowing freely in the blood stream. If it reaches the lungs and stays there a pulmonary thrombus can occur causing breathing difficulties; if it bypasses the lungs the next place it goes to is the brain putting the person at risk for a stroke and if it reaches back to the heart the patient can have a heart attack. This why you commonly see patients with atrial fibrillation on the med Coumadin or some form of anticoagulant drug to prevent clots from occurring.
An estimated 2.7 million Americans are living with Afib.
Episodes of atrial fibrillation can come and go, or you may develop atrial fibrillation that doesn’t go away and may require treatment. Although atrial fibrillation itself usually isn’t life-threatening if kept under control meaning HR under 100, it is a serious medical condition that sometimes requires emergency treatment. It can lead to complications. Atrial fibrillation may lead to blood clots forming in the heart that may circulate to other organs and lead to blocked blood flow (ischemia) to even stroke (cause the clot reached the brain or heart attack cause the clot is in the heart) to pulmonary thrombus (cause the clot reached the lungs), as stated earlier.
Treatments for atrial fibrillation may include medications like anticoagulants primarily=Coumadin, Plavix, antiplatelets=aspirin (platelets are responsible for clotting in our bloodstream) with and other interventions to try to alter the heart’s electrical system such as cardioversion-shocking the heart at low level voltage, more common in newly diagnosed afib. in hope to knock the afib into a regular rhythm called normal sinus rhythm (the best rhythm to be in). We have a normal sinus node in our right upper chamber that gives the signals for our pulsation of the heart and is the reason the best rhythm is called sinus normal rhythm.
Various studies have reported that electrical cardioversion is over 90 percent effective in converting to a normal sinus rhythm though many people revert back into afib shortly thereafter. Success has been shown to be enhanced when patients are on an anti-arrhythmic drug beforehand, which helps prevent reverting back to atrial fibrillation.
Success depends on the size of the left atrium as well as how long the patient has been in a=fib.. Patients with a very large left atrium, one greater than 5 cm, or who have been in constant a-fib for a year or two, may find that electrical cardioversion is not effective in converting to or maintaining a normal sinus rhythm (the best heart rate to be in; remember the natural pacemaker of the heart lies in our right upper side of the chamber on the lateral side not the medial side which we call the Sinus Node. The sinus rhythm derives from this sinus node, that is why its the best rhythm to be in especially if your under HR is from 60 to less than 100. Ideal HR a minute is 60-80s.).
Following a successful electrical cardioversion to treat uncontrolled atrial fibrillation (in the medical abbreviated by calling it afib also), the goal is to maintain a normal sinus rhythm, which only happens with about 20–30 percent of patients within the first year if they are not on anti-arrhythmic drugs for rhythm control. Overall, the likelihood is quite high that you will revert back into atrial fibrillation, regardless of whether you stay on rhythm control drugs.
Always remember if you remain in Atrial Fibrillation and the HR is kept under 100 with no symptoms you can live a completely normal life. Also always follow up with your cardiologist to keep an eye on your rhythm with following the M.D. treatment.
When the ventricles beat too rapidly they don’t fill completely with blood from the atria. As a result, they cannot efficiently pump blood out to meet the needs of the body. This can ultimately lead to heart failure in time if not treated. Just like us running from NY to California most will end up not being able to do it just like the heart can’t run in atrial fibrillation in a high heart rate for a long time, it also will give out going into failure. The heart can only compensate in atrial fibrillation in a rapid high heart rate for so long than stop if no treatment is done.
A cardiac condition called Rapid Ventricular Rate or Response which is seen sometimes with Atrial Fibrillation which is the heart is overloaded. Our heart beats lub dub which is first the atriums opening and closing (lub) and than the ventricles opening and closing (dub). When the heart gets overworked and tries to compensate the atriums can give up and just allow the ventricles to take over to beat which affects the heart and all other tissues to get proper amount of blood with oxygen in time. Since you loose the atriums (the upper chambers of the heart) and they don’t fill up with the amount of blood volume like they use to before having afib+. You loose a lot of blood volume(RBC’s); what the heart pumps out in the left ventricle to our tissues with oxygen get’s decreased in what we call your cardiac output=the volume of oxygenated blood pumped out of the left ventricle. Well with atrial fibrillation this gets compensated. In time if this is not repaired the blood goes backwards in how the heart pumps the blood. It is regurgitating blood back in the heart back in the pulmonary vein back to the lungs putting fluid in the lungs even going further back into the Rt side of the heart if it is reaching that far and then superior vena cava and even further depending how long this hasn’t been treated. Heart failure is set up, if not already diagnosed.
Heart failure can result of Atrial Fibrillation with RVR overtime and is the most common in those who already have another type of heart disease like CAD (Coronary Heart Disease, CHF, heart valve disease etc…).
RVR can cause chest pains and make conditions like congestive heart failure worse (they are already with a heart not functioning at its optimal). RVR is simply having a high heart rate with the ventricles only pumping. The HR can be like over 100-280. You need to get to an ER to be treated immediately. This is where you would be started on a IV drip like Cardizem to bring the HR down to get you in controlled atrial fibrillation or some type of medication in bringing the HR down to cardioverted after cleared you have no clot in your heart especially since the shock can make it loose in your bloodstream. We already reviewed earlier what a loose clot can cause. HR meaning the heart rate or pulse which just like a car if not maintained properly it will wear down till it no longer works or dies! Be could to your heart you only have one unless you get a transplant which is very hard to obtain; and why bother for if you control your a-fib it will allow you to live a completely normal life if that is your only medical or medical condition you have. Its all up to you!