“Most stings arise because an insect perceives a threat to their colony. Bees and wasps commonly sting because an intruder has neared the hive or nest.”
MEDICINENET.COM 12/11/2013 Bee and Wasp Sting
“Most stings arise because an insect perceives a threat to their colony. Bees and wasps commonly sting because an intruder has neared the hive or nest.”
MEDICINENET.COM 12/11/2013 Bee and Wasp Sting
“It is a major cause of stroke, especially in the elderly. Although the causes are diverse, hypertension is common.”
AHA (American Heart Association)

Working of the heart:
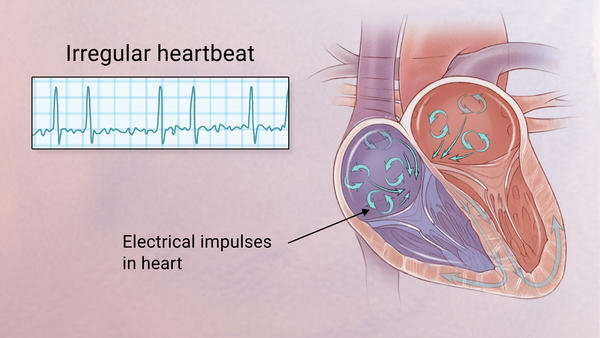
To easily identify atrial fibrillation with RVR, it is vital to understand the working of the heart. The atrium or atria (plural) is the upper chamber of the heart, bigger in size compared to the lower chambers known as the ventricles. The atria function by gathering blood as it flows into the heart and shrinking to forward the blood into the ventricles. At the very moment, the smaller ventricle must shrink to forward the blood to all parts of the body. This rhythm of blood flow creates a heart signature voice referred to as the Sinus rhythm. It is important that the sinus rhythm is synchronized so that the atrium does not send blood into the ventricle out of cue. To achieve this, an electric signal is generated to ensure the atrium contracts. When this signal short circuits (bypasses) the atrium, atrial fibrillation with RVR occurs, and the atrium is seen to vibrate just like jelly on a flat surface.
Atrial fib with RVR refers to atrial fibrillation with rapid ventricular rate. Usually the heart is like clockwork, the top (collecting) chambers beat then the bottom (main pumping) chambers sense this and also beat, and so on, in a nice regular fashion just like a clock ticking second after second. Usually the heart beats at about 60-80 beats per minute.
In atrial fibrillation the top chamber basically goes crazy often firing off over 400 beats per minute! Atrial fibrillation with RVR (Rapid Ventricular Response) is a heart condition caused by irregular electrical activity that results in irregular contractions of the 2 top heart chambers fibrillating. This means the heart (atriums), shakes with a rapid tremulous movement or makes fine irregular twitching movements, generally referred to as fibrillating causing little control in the heart output of blood by the heart but the lower chambers called the ventricles take over.
These bottom chambers don’t allow all those impulses through but it does let every second or third one through. This can give a heart rate of 100-180 beats per minute at rest, still too many beats, known as Afib with RVR, leading to symptoms and problems with heart function. Afib does not necessarily lead to Afib with RVR however, Afib can be rate controlled, sometimes naturally, sometimes using medications and sometimes requiring procedures as discussed below.
In most people with AFib although symptoms can sometimes be unpleasant it is generally not harmful as long as the afib is controlled, meaning the heart in the afib rhythm with the pulse under 100. The main concern is stroke, but that can be treated with the use of blood thinning medications in people at risk. In Afib with RVR, basically the heart is beating too fast. Of course palpitations are the most common symptom. Other symptoms of AFib with RVR may include dizziness, lack of energy, exercise intolerance and shortness of breath. If Afib with RVR goes on for too long then this may result in heart failure and of course worsening of existing heart failure. Control of the heart rate in patients with Afib with RVR often causes these symptoms to improve, again meaning the HR is under 100 with the heart rhythm in afib.
A major indication of atrial fibrillation with RVR is a very rapid heartbeat rate, although some patients are known to have the condition without showing symptoms. Atrial fibrillation with RVR may occur when cardiac muscle cells overcome their intrinsic pacemaker’s signals and fire rapidly differently from their normal pattern spreading the abnormal activity to the ventricles. The rapid heart rate can strain the heart, developing a situation referred to as Tachycardia (meaning a pulse greater than 100). Atrial fibrillation with RVR can be detected from the various symptoms though it is important to remember that some patients have experienced the condition without symptoms.
Symptoms:
Some of the symptoms of this disease include heart palpitations (described as unnoticed skipped beats or skipped beats noticed from experienced dizziness or difficulty in breathing), shortness of breath when lying flat (orthopnea), shortness of breath (dyspnea after exertion) sudden onset of short breath during the night (also called paroxysmal nocturnal dyspnea) and gradual swelling of lower extremities. As a result of inadequate blood flow, some patients complain of light headedness and may feel like they are about to faint, a condition referred to as presyncope and may actually lose consciousness (syncope). Some patients experience respiratory distress that results in them appearing blue. A close examination of jugular veins usually reveals elevated pressure in some patients (jugular venous distention). When some patients are subjected to lung examinations, crackles and rales may be observed pointing to possible lung edema.
Importance of proper diagnosis:
A good diagnosis of the symptoms shown by patients is important to ascertain that the patient is suffering from atrial fibrillation with RVR. This is because some forms or irregular and rapid heart rates, tachyarrhythmia, are dangerous and must be ruled out as they are life threatening – such as ventricular tachycardia. Some patients are usually placed on continuous cardio respiratory monitoring, but an electrocardiogram ECG is vital for correct diagnosis.
How is it diagnosed?
Simple, a typical 12 lead electrocardiogram (ECG). This test shows cardiac rhythms which atrial fibrillation is. Rhythms are made up of types of waves that the ECG shows which are P waves, QRS waves, T waves and U waves.
The QRS complexes should be narrow, to signify that they are being initiated by normal conduction of atrial electrical activity through the Intra-ventricular conduction system, or heart conduction system. Wide QRS complexes could point to ventricular tachycardia, although wide complexes may also be an indication of disease processes in the Intra-ventricular conduction system. The R-R internal will also likely be irregular. Meaning measuring from each R section of the QRS rhythm. It is also important to find out if there are triggering causes for the tachycardia which include dehydration, Hypovolemia – a decrease in blood volume, and more specifically decrease in blood plasma volume. You can go ahead to eliminate Acute coronary syndrome – which refers to any diseases that are directly attributed to the obstruction of coronary arteries.
WHAT IS THE TREATMENT:
A Shock
This is known as cardioversion and is used typically either when an immediate result is required or used when the Afib is of relatively recent onset or only intermittent, and so has more chance of staying in normal rhythm. In cardioversion a small shock is given using defibrillation pads. It is done under light anesthesia therefore it doesn’t hurt. The Afib may return however.
Rate Control Drugs
The biggest problem in Afib with RVR is too fast a heart rate. In a rhythm control strategy we use drugs such as beta-blockers to slow the heart rate down. These drugs typically will leave the patient in AF. For many people with AF it turns out that a rate control strategy is preferred as it is considered less risky than the rhythm control drugs used to get rid of the AF while being just as effective. In Afib with RVR rate control drugs can often slow the heart rate down fairly quickly and improve symptoms.
Rhythm Control Drugs
These medications are generally more powerful than the rate control drugs and attempt to convert the Afib back in to a normal rhythm. They are often given after a shock treatment to try and help the heart stay in normal rhythm. These drugs are also commonly used in hospitalized Afib with RVR patients. The problem with these drugs is that they may have side effects and associated risks. Many patients simply cannot tolerate Afib even if the rate is controlled and therefore require rhythm control drugs. They may be safe and effective however if used in selected patients. In cases of Afib with RVR these medications may need to be used if patients cannot tolerate other rate control medications.
Ablation Procedures
Ablation procedures are minimally invasive procedures typically done through the groin. They are typically used in patients that have tried, or cannot tolerate medicines for control of AFib. Ablation is typically not used as an emergency treatment of Afib with RVR, rather it is used for stable patients in AF, or those with intermittent AFib that wish to remain in normal rhythm. In patients that have had persistent Afib for a long time these procedures are not likely to be successful in the long term.
Pacemaker
This is typically the last throw of the dice for AF control. In some patients, drugs can either not control the rate in AFib with RVR, or the drugs can simply not be tolerated. In these patients who have no other choice, and in whom it is determined the Afib is causing harmful effects, a procedure called AV node ablation and pacemaker is done. In a relatively minor procedure, a small burn is made to the connection that connects the top and bottom chambers of the heart. A pacemaker is then inserted. This prevents Afib with RVR as although the top chambers continue to fire at a fast rate, the pacemaker now controls the bottom chamber, in a nice regular way. The downside of course is that now although the patient cannot have Afib with RVR, they have a pacemaker.
Acute afib RVR patients are more likely to be converted to Normal Sinus Rhythm (the best rhythm you could be in) as opposed to patients with chronic afib. There are complete resolutions for both kind of afib but atrial fibrillation in RVR the heart can handle for only so long and remembering the engine of our body is the heart so take good care of it for if you don’t it could allow you to die.
“When you exhaust all possibilities remember this: You haven’t!”
Thomas Edison (Inventor and Businessman)
“But the key to our marriage is the capacity to give each other a break. And to realize that it’s not how our similarities work together; it’s how our differences work together.”
Michael J. Fox (Actor & spokesman for Parkinson’s Disease)
How to care for IBS:
1. IBS Treatment through Diet
2. IBS Treatment through Supplements
3. IBS Treatment through Alternative Therapies
4. IBS Treatment through Stress Management
5. IBS Treatment through Prescription Medications
Help from IBS.com
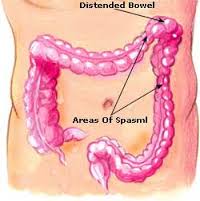
Irritable bowel syndrome is a group of symptoms – including abdominal pain and changes in the pattern of bowel movements without any evidence of underlying damage. These symptoms occur over a long time, often years. It has been classified into four main types depending on if diarrhea is common, constipation is common, both are common, or neither occurs very often. IBS negatively affects quality of life and may result in missed school or work. Disorders such as anxiety, major depression, and chronic fatigue syndrome, are common among people with IBS.
Treatments and drugs
Because it’s not clear what causes irritable bowel syndrome, treatment focuses on the relief of symptoms so that you can live as normally as possible.
In most cases, you can successfully control mild signs and symptoms of irritable bowel syndrome by learning to manage stress and making changes in your diet and lifestyle. Try to avoid foods that trigger your symptoms. Also try to get enough exercise, drink plenty of fluids and get enough sleep.
If your problems are moderate or severe, you may need more than lifestyle changes. Your doctor may suggest medications.
Dietary changes:
“A study just published by Clinicians on patients in the West Midlands who travelled overseas to receive Living Donor transplants has found that clinical outcomes are often poor. Over 30% of the patients in the study who travelled either died within three months (17%) or lost their new kidney within a year(14%).”
National Kidney Federation
When people languish on a wait-list for a kidney transplant, they may start to consider a desperate measure: Traveling to a country where they can buy a donor kidney on the black market.
But beyond the legal and ethical pitfalls, experts say, the health risks are not worth it.
Most countries ban the practice, sometimes called “transplant tourism,” and it has been widely condemned on ethical ground. Now a new study highlights another issue: People who buy a donor kidney simply do not fare as well.
Researchers in Bahrain found that people who traveled abroad to buy a kidney — to countries like the Philippines, India, Pakistan, China and Iran — sometimes developed serious infections.
Those infections included the liver diseases hepatitis B and C, as well as cytomegalovirus, which can be life-threatening to transplant recipients, the investigators said.
Also, people who bought donor kidneys also faced higher rates of surgical complications and organ rejection, versus those who received a legal transplant in their home country.
Dr. Amgad El Agroudy, of Arabian Gulf University, was to present the findings Friday at the annual meeting of the American Society of Nephrology (ASN), in San Diego.
It’s not clear how common it is for U.S. patients to take a chance on traveling abroad to buy a black-market kidney, according to Dr. Gabriel Danovitch, director of kidney transplantation at the University of California, Los Angeles.
“We really have no way of knowing what the numbers are,” said Danovitch, who was not involved in the study.
“But,” he added, “my sense is that the numbers are fairly small, as the dangers of transplant tourism are becoming more and more clear.”
Why is it a risky proposition? According to Danovitch, there are a few broad reasons: The paid organ donors may not be properly screened, and the recipients may not be good candidates for a transplant, to name two.
“In a paid system, the prime focus is on making money,” Danovitch said. “Centers that are willing to do these don’t really care what happens to the donors or recipients after the transplant.”
For people with advanced chronic kidney failure, the treatment options are dialysis or a transplant. But there are not enough donor organs to meet the need. In the United States, nearly one million people have end-stage kidney disease, and there are roughly 102,000 people on the waiting list for a transplant, according to the National Kidney Foundation.
Kidney transplants can come from a living or deceased donor, but living-donor transplants are more likely to be successful, according to U.S. health officials.
It doesn’t take long to get tired of spending 12 hours a week on hemodialysis, or even more time on peritoneal dialysis (PD) —not to mention complications like line infections and access problems. But a new, healthy kidney would put an end to all that. A transplant sounds like it would be well worth the risk of surgery and the trouble of taking anti-rejection medicines, and Medicare statistics show that it actually costs less in the long run than continued dialysis. When can you check into the hospital, you ask?
Unfortunately over 80,000 people in the United States are already waiting for a new kidney and in 2008 only 16,517 got one. Maybe you don’t have a compatible donor in your family, or you’ve been told that you are “not a transplant candidate” for one of several reasons. You’re a resourceful person who knows that persistence pays off, and you start looking for ways to shorten the wait or get around the rules that say you don’t qualify for a transplant. Kidneys from living donors are almost always preferable to those from recently deceased donors. If you don’t have a friend or family member willing to donate, what about getting one where the laws against buying an organ are less strictly enforced? Medical tourism is booming these days. Maybe you know somebody who had surgery overseas, either to avoid a waiting list or just because the price is lower there. The same international pharmaceutical countries produce medicines for everybody these days, so how big a difference can there be? Nephrologists in the US say it’s a common story: a dialysis patient misses treatments or appointments for a few days or several weeks, then comes to their office asking for refills on anti-rejection medicines…with pill bottles labeled in Urdu, Chinese or Farsi as well as in English. Did they get a good deal or what? Unfortunately this may not be the bargain people hoped for.
At UCLA Jagbir Gill, MD, and associates studied 33 patients who had received transplants overseas, and found they had much worse results than patients who received transplants in this country. Screening of paid kidney donors was less thorough, with problems like hepatitis overlooked. Early organ rejection was twice as common and infections frequent; Dr. Gill recalls patients who went “directly from the airport to the emergency room” due to severe infections or transplant failure.
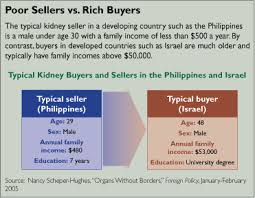
In a similar study in Canada, where waiting periods for transplants are even longer, experiences were similar. Jeffrey Zaltzman, MD, reports infections common in the countries where the transplant was done were a big problem in medical tourists. One 78-year-old gentleman returned from Pakistan with a surgical wound that reopened spontaneously; he died a few weeks later of cardiovascular problems that might have disqualified him for a transplant at home. The cost to paid organ donors can be even greater. Poor people who sell a kidney, sometimes for as little as $800 according to the World Health Organization, face health problems like hypertension and worsening of their own kidney functions—provided, of course, that their surgery goes well. Since most live in countries where even blood pressure checks are rare, complications that develop after they leave the hospital may go undetected until it is too late for the patient. Donors in the United States frequently can have kidneys removed with very small incisions. Third World donors, however, generally end up with wounds up to 14 inches long that may take months to heal, making them unable to do the manual labor most depend on. Chronic pain and disability are common, points out Nancy Scheper-Hughes, who has extensively studied and reported on transplant practices from Brazil to China. And reports of organs coming from executed prisoners in China are even more worrisome. Details of where donors come from and which hospitals and doctors will do the surgery are rarely available to “clients” and their families ahead of time. While paying a donor for an organ is illegal everywhere except Iran, “international transplant coordinators” have no laws banning what they do—bringing clients together with hospitals in other countries. And as the WHO’s Dr. Luc Noel points out, “None of the brokers ever mention the costs—long-term health issues, chronic pain, inability to perform manual labor—that are borne by these poor organ vendors.”
SO THINK TWICE BEFORE FALLING FOR TRANSPLANT TOURISM. HIGH PROBABILITY YOU WON’T LIKE THE RESULTS!
“2 ways to replace the kidneys: Hemodialysis cleans and filters your blood using a machine to temporarily rid your body of harmful wastes, extra salt, and extra water. Hemodialysis helps control blood pressure and helps your body keep the proper balance of important chemicals such as potassium, sodium, calcium, and bicarbonate. Peritoneal dialysis is another procedure that removes wastes, chemicals, and extra water from your body. This type of dialysis uses the lining of your abdomen, or belly, to filter your blood.”
National Institute of Diabetes and Digestive and Kidney Diseases