3X7340
What are enzymes?
Enzymes are vital for processes to take place in our body without them they couldn’t take place. We have many enzymes in our body from our saliva to our pancreas. Enzymes are specialized proteins that are produced by living cells to catalyze reactions in the body=breakdown.
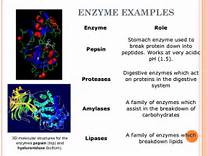
A catalyst in action brakes down something, any chemical substance affected with the speed of reaction without being permanently altered by the reaction. For a chemical or biochemical reaction to occur, a certain amount of energy is required=the activation energy. Energy can be transformed from one state to another. The role of an enzyme is to decrease the amount of energy needed to start the reaction. Exactly how enzymes lower activation energies is not completely and fully understood but it is known that an enzyme attaches itself to one of the reacting molecules, this is called a substrate complex. Thousands of enzymes exist but each kind can attach ONLY to one kind of substrate. The enzyme molecule must fit exactly with the substrate molecule (just like how pieces in a jigsaw puzzle have to fit in their specific space of the picture). Well, if the substrate and enzyme don’t perfectly match or fit properly no reaction takes place. When they do fit perfectly the substrate molecule can react with other molecules in a synthesis reaction and when completed the enzyme is free to move on elsewhere to connect with another substrate molecule. This whole process takes place quickly. Clearly, enzymes are essential to the body’s overall homeostasis. (In order to lead a healthy life, we need to bring a balance in the way we lead our lifestyle. Homeostasis is nothing but a mechanism which helps the human body maintain a balance between the internal and external environment). Enzymes quickly perform catalyze chemical reactions and they also govern the reactions that occur. Enzymes are named by adding the suffix “ase” to the name of their substrates. Here are some examples below.
Protein in the form of an enzyme acts as a catalyst.
The breaking down of proteins=Trypsin Proteins are large biological molecules consisting of one or more chains of amino acids. Proteins perform a vast array of functions within living organisms, including catalyzing metabolic reactions, replicating DNA, responding to stimuli, and transporting molecules from one location to another. Trypsin is a enzyme catalyst, which allows the catalysis of chemical reactions. The ending product of the break down is amino acids not sugar. Know high on a protein diet continuously for years can hurt the body also.
The breaking down of starches = the enzyme that does this function is amylase
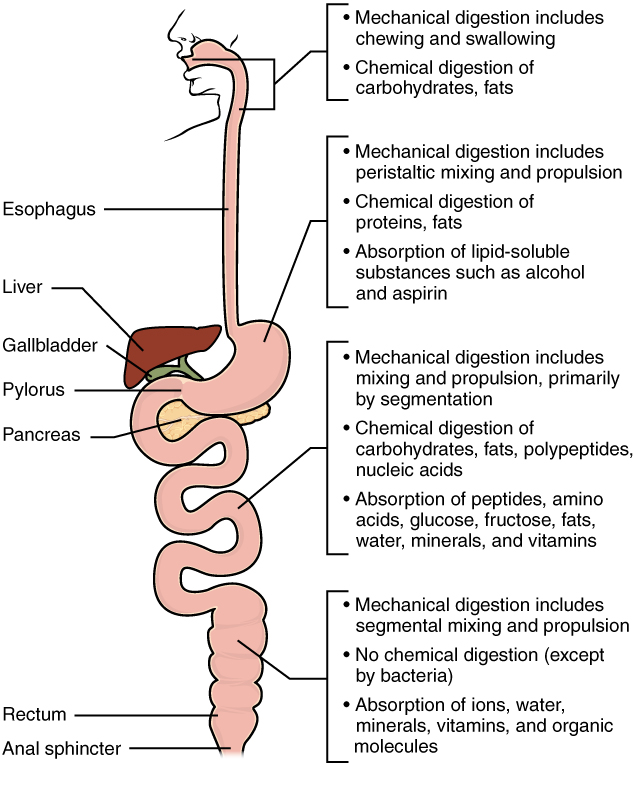
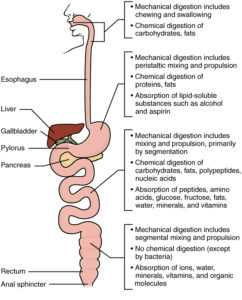
Know this about amylase, it is present in human saliva where it begins the chemical process of digestion; that starts in our mouth. Foods that contain much starch but little sugar, such as rice and potato, taste slightly sweet as they are chewed because amylase turns some of their starch into sugar in the mouth. The pancreas also makes amylase (alpha amylase) to hydrolyse dietary starch into disaccharides and trisaccharides which are converted by other enzymes to glucose to supply the body with energy. There is even b and y amylases. Ending product on enzymes breaking down starches or carbohydrates gives us one thing only sugar.)
The breaking down of sugars, like sucrose = the enzyme is sucrase. The ending product of the enzyme is it breaks down complex sugars to more simple sugars in the body.
The breaking down of fats (lipids) = the enzyme is lipase.
Lipase perform essential roles in the digestion, transport and processing of dietary lipids in most if not all living organisms (example (triglycerides, fats, oils).Most lipases act at a specific position on glycerol backbone of lipid substrate (A1,A2 or A3 in the small intestines). For example, human pancreatic lipase (HPL) is the main enzyme that breaks down dietary fats in the digestive system, converts triglyceride substrates found in ingested oils to monoglycerides and two fatty acids. Know that glycerol is a simple sugar compound. Enzymes deal with breaking down our foods because they take a major role in what we call the process digestion in the human body but notice what the ending result is of mostly every ingredient out of 3 of our food groups, which is SUGAR. It’s because of the food already having some sugar in it but more importantly also the chemical reaction with the enzyme to allow the food to break down into smaller compounds to be utilized in the body=simpler sugar compounds which also plays a part in the entire digestion process.
So know sugar in the body is our fuel for energy with the help of digestion process to breakdown sugars, this is how it work:
When the body gets a meal within 1 hour digestion starts in the stomach and complete in 6 to 8 hours depending on how large the meal is, especially if 3 large meals a day. The foods if contain starches, fat, lipids they all break down to simple sugars that transfer to the bloodstream and whatever energy the body needs at that point the tissues with cells utilize it but when enough sugar is used and we have excess in the blood we than have the body store the extra sugar that first converts the glucose (active sugar) to glycogen (inactive sugar) in our liver. The liver is only so big and when it reaches its optimal level of storage than the sugar gets stored in our fat tissue = WEIGHT GAIN. This is the problem with people in America not understanding this process. Plus as most people get older from 30 than to 40 years old and every 10 years after that till heaven we put cellulite on the body for 2 major reasons not eating as healthy due to the bikini and speedo fit not being the priority in life but getting the feet up after a hard day’s work is. The other reason is we aren’t as active as when we were 20 or 30 years old and the metabolism naturally slows down unless you’re a Jack la Lanne or body trainer.
How do we deal with this to prevent obesity? Do what I did go on a 4-6 small meal/health snack diet. Eat a meal every 3 hours with keeping fat, calories/sugar, carbohydrates in proper proportions to prevent excess sugar in the meals to not allow fat storage=weight gain. Of course some exercise or activity daily or every other day helps tone the muscle and not let it flab due to cellulite. Live healthier habits of living not just a month, 3 months or 6 months but make it your daily routine with treating yourself to foods you don’t eat daily to maintain a good weight and increase your health status to allow you to live a happier, longer and more exciting life.
Enzymes deal with breaking down our foods because they take a major role in what we call the process digestion in the human body. but notice what the ending result is of mostly every ingredient in our 4 food groups is; SUGAR. It because of the food has some sugar in it but also the chemical reaction with the enzyme to allow the food to break down into smaller compounds to be utilized in the body with send through the entire digestion process.
There are risks with eating just high protein diets for long periods of time. You put yourself at risk for: Osteoporosis: Research shows that women who eat high protein diets based on meat have a higher rate of bone density loss than those who don’t. Women who eat meat lose an average of 35% of their bone density by age 65, while women who don’t eat meat lose an average of 18%. In the long run, bone density loss leads to osteoporosis.
Kidneys: A high protein diet puts strain on the kidneys. It is well known that patients with kidney problems suffer from eating a high protein diet which is due to the high amino acids levels. A high-protein diet may worsen kidney function in people with kidney disease because your body may have trouble eliminating all the waste products of protein metabolism.
However, the risks of using a high-protein diet with carbohydrate restriction for the long term are still being studied. Several health problems may result if a high-protein diet is followed for an extended time:
Some high-protein diets restrict carbohydrate intake so much that they can result in nutritional deficiencies or insufficient fiber, which can cause health problems such as constipation and diverticulitis.
Some high-protein diets promote foods such as red meat and full-fat dairy products, which may increase your risk of heart disease.
If you want to follow a high-protein diet, do so only as a short-term weight-loss aid. Also, choose your protein wisely. Good choices include fish, skinless chicken, lean beef, pork and low-fat dairy products. Choose carbs that are high in fiber, such as whole grains and nutrient-dense vegetables and fruit.
It’s always a good idea to talk with your doctor before starting a weight-loss diet. And that’s especially important in this case if you have kidney disease, diabetes or other chronic health condition.
So if you want to continue on high protein diets longer than 6 months know how to alkalize the body chemicals to decrease the proteins and there are supplements that can do that via the pharmacy or look up even online.
Before changing your diet always do a diet check with your doctor to make sure its cleared “OK” by the doctor since he knows your entire medical history!