Impact of pets on human health.


 The effects of Human Animal Interaction-HAI on psychosocial variables such as empathy and social interactions and on human physical and mental health, including effects on hormones and the autonomic nervous system assessed via variables such as heart rate or blood pressure. Effects could result from either companion animal ownership or animal contacts, in experimental settings or animal-assisted interventions. Studies not directly related to these topics were excluded, for example, on pet ownership and attitudes toward smoking, or other variables which could indirectly influence health or social contacts (e.g., Milberger et al., 2009; Zimolag and Krupa, 2009). From several hundred publications found via the terms “pet,” “cat,” or “dog” include relevant original research articles (see Table 1 below at www.ncbi.nim.nih.gov/pmc/articles) as well as reviews and meta-analyses. Animals play an important role in many people’s lives. In addition to seeing-eye dogs and dogs that can be trained to detect seizures, animals can also be used in occupational therapy, speech therapy, or physical rehabilitation to help patients recover. Aside from these designated therapeutic roles, animals are also valued as companions, which can certainly affect the quality of our lives. Is that companionship beneficial to our health? The better we understand the human-animal bond, the more we can use it to improve people’s lives. Over 71 million American households (62%) have a pet, and most people think of their pets as members of the family.3 Some research studies have found that people who have a pet have healthier hearts, stay home sick less often, make fewer visits to the doctor, get more exercise, and are less depressed. Pets may also have a significant impact on allergies, asthma, social support, and social interactions with other people. Impact on Physical Health Companion animals may improve heart health by lowering blood pressure and regulating the heart rate during stressful situations. In a 2002 study, researchers measured changes in heart rate and blood pressure among people who had a dog or cat, compared to those who did not, when participants were under stress (performing a timed math task). People with a dog or cat had lower resting heart rates and blood pressure measures at the beginning of the experiment than non-pet owners. People with a dog or cat were also less likely to have spikes in heart rates and blood pressure while performing the math task, and their heart rates and blood pressure returned to normal more quickly. They also made fewer errors in their math when their pet was present in the room. All these findings indicated that having a dog or cat lowered the risk of heart disease, as well as lowering stress so that performance improved. A similar study found that having your dog in the room lowered blood pressure better than taking a popular type of blood pressure medication (ACE inhibitor) when you are under stress. Children’s exposure to companion animals may also ease anxiety. For example, one study measured blood pressure, heart rate, and behavioral distress in healthy children aged 3 to 6 at two different doctor visits for routine physicals. At one visit a dog (unrelated to the child) was present in the room and at the other visit the dog was absent. When the dog was present, children had lower blood pressure measures, lower heart rates, and less behavioral distress. Research on the health benefits of child and animal interaction is limited. Further research is needed on how pets influence child development and specific health outcomes. These findings suggest that the social support a pet provides can make a person feel more relaxed and decrease stress. Social support from friends and family can have similar benefits, but interpersonal relationships often cause stress as well, whereas pets may be less likely to cause stress. The social support provided by a pet might also encourage more social interactions with people, reducing feelings of isolation or loneliness. For example, walking with a dog has been found to increase social interaction, especially with strangers, compared to walking without a dog. Among elderly people, pet ownership might also be an important source of social support that enhances well-being. In one study, elderly individuals that had a dog or cat were better able to perform certain physical activities deemed “activities of daily living,” such as the ability to climb stairs; bend, kneel, or stoop; take medication; prepare meals; and bathe and dress oneself. There were not significant differences between dog and cat owners in their abilities to perform these activities. Neither the length of time of having a dog or cat nor the level of attachment to the animal influenced performance abilities. Companion animals did not seem to have an impact on psychological health but researchers suggested that a care-taking role may give older individuals a sense of responsibility and purpose that contributes to their overall well-being.
The effects of Human Animal Interaction-HAI on psychosocial variables such as empathy and social interactions and on human physical and mental health, including effects on hormones and the autonomic nervous system assessed via variables such as heart rate or blood pressure. Effects could result from either companion animal ownership or animal contacts, in experimental settings or animal-assisted interventions. Studies not directly related to these topics were excluded, for example, on pet ownership and attitudes toward smoking, or other variables which could indirectly influence health or social contacts (e.g., Milberger et al., 2009; Zimolag and Krupa, 2009). From several hundred publications found via the terms “pet,” “cat,” or “dog” include relevant original research articles (see Table 1 below at www.ncbi.nim.nih.gov/pmc/articles) as well as reviews and meta-analyses. Animals play an important role in many people’s lives. In addition to seeing-eye dogs and dogs that can be trained to detect seizures, animals can also be used in occupational therapy, speech therapy, or physical rehabilitation to help patients recover. Aside from these designated therapeutic roles, animals are also valued as companions, which can certainly affect the quality of our lives. Is that companionship beneficial to our health? The better we understand the human-animal bond, the more we can use it to improve people’s lives. Over 71 million American households (62%) have a pet, and most people think of their pets as members of the family.3 Some research studies have found that people who have a pet have healthier hearts, stay home sick less often, make fewer visits to the doctor, get more exercise, and are less depressed. Pets may also have a significant impact on allergies, asthma, social support, and social interactions with other people. Impact on Physical Health Companion animals may improve heart health by lowering blood pressure and regulating the heart rate during stressful situations. In a 2002 study, researchers measured changes in heart rate and blood pressure among people who had a dog or cat, compared to those who did not, when participants were under stress (performing a timed math task). People with a dog or cat had lower resting heart rates and blood pressure measures at the beginning of the experiment than non-pet owners. People with a dog or cat were also less likely to have spikes in heart rates and blood pressure while performing the math task, and their heart rates and blood pressure returned to normal more quickly. They also made fewer errors in their math when their pet was present in the room. All these findings indicated that having a dog or cat lowered the risk of heart disease, as well as lowering stress so that performance improved. A similar study found that having your dog in the room lowered blood pressure better than taking a popular type of blood pressure medication (ACE inhibitor) when you are under stress. Children’s exposure to companion animals may also ease anxiety. For example, one study measured blood pressure, heart rate, and behavioral distress in healthy children aged 3 to 6 at two different doctor visits for routine physicals. At one visit a dog (unrelated to the child) was present in the room and at the other visit the dog was absent. When the dog was present, children had lower blood pressure measures, lower heart rates, and less behavioral distress. Research on the health benefits of child and animal interaction is limited. Further research is needed on how pets influence child development and specific health outcomes. These findings suggest that the social support a pet provides can make a person feel more relaxed and decrease stress. Social support from friends and family can have similar benefits, but interpersonal relationships often cause stress as well, whereas pets may be less likely to cause stress. The social support provided by a pet might also encourage more social interactions with people, reducing feelings of isolation or loneliness. For example, walking with a dog has been found to increase social interaction, especially with strangers, compared to walking without a dog. Among elderly people, pet ownership might also be an important source of social support that enhances well-being. In one study, elderly individuals that had a dog or cat were better able to perform certain physical activities deemed “activities of daily living,” such as the ability to climb stairs; bend, kneel, or stoop; take medication; prepare meals; and bathe and dress oneself. There were not significant differences between dog and cat owners in their abilities to perform these activities. Neither the length of time of having a dog or cat nor the level of attachment to the animal influenced performance abilities. Companion animals did not seem to have an impact on psychological health but researchers suggested that a care-taking role may give older individuals a sense of responsibility and purpose that contributes to their overall well-being.
QUOTE ON MONDAY:
Facts on smoking.
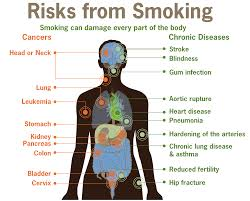

Know when the lungs get effected in time the heart gets effected. One Affects the other in time. The heart can’t live without the lungs and viCE versa.
Now knowing just this you’ll understand why smoking alone can cause the following conditions, Through the Centers for Disease Control and Prevention. They state the following:
Smoking and Increased Health Risks
Compared with nonsmokers, smoking is estimated to increase the risk of—
-
Coronary heart disease by 2 to 4 times, (causing atherosclerosis=thickening of the vessels or due to arteriosclerosis=hardening of the arteries and remember smoking causes vasoconstriction of the vessels = increase pressure in the vessels = high B/P.
-
Stroke by 2 to 4 times (Due to causing the above problems listed under coronary heart disease.)
-
Men developing lung cancer by 23 times,
-
Women developing lung cancer by 13 times(cancers due to constant irritation of the tissues) , and
-
Dying from chronic obstructive lung diseases (such as chronic bronchitis and emphysema) by 12 to 13 times. ( Explained at the top)
Smoking and Cardiovascular Disease
-
Smoking causes coronary heart disease, the leading cause of death in the United States.
-
Cigarette smoking causes reduced circulation by narrowing the blood vessels (arteries) and puts smokers at risk of developing peripheral vascular disease (i.e., obstruction of the large arteries in the arms and legs that can cause a range of problems from pain to tissue loss or gangrene) This pain to gangrene to amputation is due to lack of oxygenated blood getting to the tissue caused by the vasoconstriction the cigarette smoking caused.
-
Smoking causes abdominal aortic aneurysm (i.e., a swelling or weakening of the main artery of the body—the aorta—where it runs through the abdomen). An aneurysm with constant vasoconstriction (increases pressure) puts the aneurysm at risk for rupture because the aneurysm area isn’t as strong as the other vessels=Rupture of the aortic aneurysm
Smoking and Respiratory Disease
-
Smoking causes lung cancer.
-
Smoking causes lung diseases (e.g., emphysema, bronchitis, chronic airway obstruction) by damaging the airways and alveoli (i.e., small air sacs) of the lungs.
Smoking and Cancer
Smoking causes the following cancers: (in alphabetical order)
-
Acute myeloid leukemia
-
Bladder cancer
-
Cancer of the cervix
-
Cancer of the esophagus
-
Kidney cancer
-
Cancer of the larynx (voice box)
-
Lung cancer
-
Cancer of the oral cavity (mouth)
-
Pancreatic cancer
-
Cancer of the pharynx (throat)
-
Stomach cancer
Smoking and Other Health Effects
Smoking has many adverse reproductive and early childhood effects, including increased risk for—
-
Infertility
-
Preterm delivery
-
Stillbirth
-
Low birth weight
-
Sudden infant death syndrome (SIDS).1,2,9Smoking is associated with the following adverse health effects:1
-
Postmenopausal women who smoke have lower bone density than women who never smoked.
-
Women who smoke have an increased risk for hip fracture than women who never smoked.
QUOTE FOR THE WEEKEND:
“A stent is placed in an artery as part of a procedure called percutaneous coronary intervention (PCI) or coronary angioplasty. PCI restores blood flow through narrow or blocked arteries.”
NATIONAL HEART, LUNG AND BLOOD INSTITUTE
QUOTE FOR FRIDAY:
”A stent is placed in an artery as part of a procedure called percutaneous coronary intervention (PCI), also known as coronary angioplasty.”
NATIONAL HEART, LUNG AND BLOOD INSTITUTE
QUOTE FOR THURSDAY:
If you just do a Google search and type in ‘smoking’ or ‘lung cancer’, you will be barraged with never ending facts and numbers, like how one in every three Americans is affected by lung disease and how COPD is the third leading cause of death and if you get lung cancer the odds are 95% that you will die.
Matthew Gray Gubler ( (born March 9, 1980) is an American actor, director, fashion model, painter, and filmmaker. Best know for being in Criminal Minds.
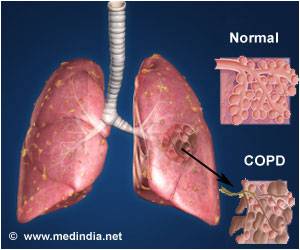
WHAT IS COPD?
Chronic Obstructive Pulmonary Disease (COPD) is largely preventable. Yet it affects over 15 million Americans and is the fourth leading cause of death in the U.S. Although many diseases have seen a gradual decline in their associated mortality, COPD rates have increased. The term COPD is a broad one used to describe a set of symptoms, referring to persistent, slowly progressive obstruction of airflow and dyspnea, that is predominantly irreversible. It may be caused by chronic bronchitis, emphysema, or bronchiectasis.
People with COPD experience deterioration in functional status; therefore, improving function is a major goal of treatment. Nurses are often facilitators and coordinators of pulmonary rehabilitation. Evaluation of the effects of treatment is an essential aspect of providing quality care. Although some effects of COPD are permanent, you can do plenty to assist your patient in managing it, by educating him on how to gain back control of his health. This will help to decrease the depression, hopelessness, and pessimism that are commonly seen in patients with COPD.
Your specific nursing measures can help ease your patient’s breathing and prevent further deterioration, thus protecting the remaining lung function and offering a better quality of life.
(Please note that asthma as not been covered extensively In this study. Only the summarization has been covered.)
Definitions, Anatomy & Pathology Review
Chronic obstructive pulmonary disease (COPD) is a term that applies to patients with chronic bronchitis, bronchiectasis, emphysema and, to a certain extent, asthma. A brief review of normal functional anatomy will provide a background for the discussion of pathology.
The airway down to the bronchioles normally is lined with ciliated pseudo-stratified columnar cells and goblet cells. Mucus derives from mucus glands that are freely distributed in the walls of the trachea and bronchi. The cilia sweep mucus and minor debris toward the upper airway. Low humidity, anesthesia gases, cigarette smoking and other chemical irritants paralyze the action of these cilia. The mucociliary action starts again after a matter of time. This is why people awaken to “smokers cough.”
“Chronic obstructive pulmonary disease (COPD) is a term that applies to patients with chronic bronchitis, bronchiectasis, emphysema and, to a certain extent, asthma.”
Bronchi run in septal connective tissue, but bronchioles are suspended in lung parenchyma by alveolar elastic tissue. The elastic tissue extends throughout alveolar walls, air passages, and vessels, connecting them in a delicate web. Bronchiolar epithelium is ciliated, single-layered and columnar or cuboidal. Beyond the bronchioles the epithelium is flat and lined with a film of phospholipid (surfactant), which lowers surface tension and thereby helps to keep these air spaces from collapsing. Remember that the phospholipid develops during later gestation in utero. This is the reason why premature infant’s lungs cannot stay inflated without the addition of surfactant therapy. Macrophages are found in alveolar lining. Smooth muscles surround the walls of all bronchi, bronchioles, and alveolar ducts and when stimulated they shorten and narrow the passages. Cartilage lends rigidity and lies in regular horse-shaped rings in the tracheal wall. Cartilage is absent in bronchi less than 1 mm in diameter.
The terminal bronchiole is lined with columnar epithelium and is the last purely conducting airway. An acinus includes a terminal bronchiole and its distal structures. Five to ten acini together constitute a secondary lobule, which is generally 1 to 2 cm in diameter and is partly surrounded by grossly visible fibrous septa. Passages distal to the terminal bronchiole include an average of three but as many as nine generations of respiratory bronchioles lined with both columnar and alveolar epithelium. Each of the last respiratory bronchioles gives rise to about six alveolar ducts, each of these to one or two alveolar sacs, and finally each of the sacs to perhaps seventy-five alveoli. Alveolar pores (pores of Kohn) may connect alveoli in adjacent lobules.
Two different circulations supply the lungs. The pulmonary arteries and veins are involved in gas exchange. The pulmonary arteries branch with the bronchi, dividing into capillaries at the level of the respiratory bronchiole, and supplying these as well as the alveolar ducts and alveoli. In the periphery of the lung, the pulmonary veins lie in the interlobular septa rather than accompanying the arteries and airways. The bronchial arteries are small and arise mostly from the aorta. They accompany the bronchi to supply their walls. In some cases of COPD, like bronchiectasis, extensive anastomoses develop between the pulmonary and bronchial circulations. This can allow major shunting and recirculation of blood, therefore contributing to cardiac overload and failure. Lymphatics run chiefly in bronchial walls and as a fine network in the pleural membrane. The lumina of the capillaries in the alveolar walls are separated from the alveolar lining surfaces by the alveolar-capillary membrane, consisting of thin endothelial and epithelial cells and a minute but expansile interstitial space. This interface between air and blood, only 2 microns in thickness, is the only place where gases may be exchanged effectively.
Diseases that make up COPD:
Chronic Bronchitis
Chronic bronchitis is a clinical disorder characterized by excessive mucus secretion in the bronchi. It was traditionally defined by chronic or recurrent productive cough lasting for a minimum of three months per year and for at least two consecutive years, in which all other causes for the cough have been eliminated. Today’s definition remains more simplistic to include a productive cough progressing over a period of time and lasting longer and longer. Sometimes, chronic bronchitis is broken down into three types: simple, mucopurulent or obstructive. The pathologic changes consist of inflammation, primarily mononuclear, infiltrate in the bronchial wall, hypertrophy and hyperplasia of the mucus-secreting bronchial glands and mucosal goblet cells, metaplasia of bronchial and bronchiolar epithelium, and loss of cilia. Eventually, there may be distortion and scarring of the bronchial wall.
Asthma
Asthma is a disease characterized by increased responsiveness of the trachea and bronchi to various stimuli (intrinsic or extrinsic), causing difficulty in breathing due to narrowing airways. The narrowing is dynamic and changes in degree. It occurs either spontaneously or because of therapy. The basic defect appears to be an altered state of the host, which periodically produces a hyperirritable contraction of smooth muscle and hypersecretion of bronchial mucus. This mucus is abnormally sticky and therefore obstructive. In some instances, the illness seems related to an altered immunologic state.
Histological changes of asthma include an increase in the size and number of the mucosal goblet cells and submucosal mucus glands. There is marked thickening of the bronchial basement membrane and hypertrophy of bronchial and bronchiolar smooth muscle tissue. A submucosal infiltration of mononuclear inflammatory cells, eosinophils and plugs of mucus blocks small airways. Patients who have had asthma for many years may develop cor pulmonale and emphysema.
Emphysema
Pulmonary emphysema is described in clinical, radiological and physiologic terms, but the condition is best defined morphologically. It is an enlargement of the air spaces distal to the terminal non-respiratory bronchiole, with destruction of alveolar walls.
Although the normal lung has about 35,000 terminal bronchioles and their total internal cross-sectional area is at least 40 times as great as that of the lobar bronchi, the bronchioles are more delicate and vulnerable. Bronchioles may be obstructed partially or completely, temporarily or permanently, by thickening of their walls, by collapse due to loss of elasticity of the surrounding parenchyma, or by influx of exudate. In advanced emphysema, the lungs are large, pale, and relatively bloodless. They do not readily collapse. They many contain many superficial blebs or bullae, which occasionally are huge. The right ventricle of the heart is often enlarged (cor pulmonale), reflecting pulmonary arterial hypertension. Right ventricular enlargement is found in about 40% of autopsies of patients with severe emphysema. The distal air spaces are distended and disrupted, thus excessively confluent and reduced in number. There may be marked decrease in the number and size of the smaller vascular channels. The decrease in alveolar-capillary membrane surface area may be critical. Death may result from infection that obliterates the small bronchi and bronchioles. There is often organized pneumonia or scarring of the lung parenchyma due to previous infections.
Classification of emphysema relies on descriptive morphology, requiring the study of inflated lungs. The two principal types are centrilobular and panlobular emphysema. The two types may coexist in the same lung or lobe.
Centrilobular emphysema (CLE) or centriacinar emphysema affects respiratory bronchioles selectively. Fenestrations develop in the walls, enlarge, become confluent, and tend to form a single space as the walls disintegrate. There is often bronchiolitis with narrowing of lumina. The more distal parenchyma (alveolar ducts and sacs and alveoli) is initially preserved, then similarly destroyed as fenestrations develop and progress.
The disease commonly affects the upper portions of the lung more severely, but it tends to be unevenly distributed. The walls of the emphysematous spaces may be deeply pigmented. This discoloration may represent failure of clearance mechanisms to remove dust particles, or perhaps the pigment plays an active role in lung destruction. CLE is much more prevalent in males than in females. It is usually associated with chronic bronchitis and is seldom found in nonsmokers.
Panlobular emphysema (PLE) or panacinar emphysema is a nearly uniform enlargement and destruction of the alveoli in the pulmonary acinus. As the disease progresses, there is gradual loss of all components of the acinus until only a few strands of tissue, which are usually blood vessels, remain. PLE is usually diffuse, but is more severe in the lower lung areas. It is often found to some degree in older people, who do not have chronic bronchitis or clinical impairment of lung function. The term senile emphysema was formerly applied to this condition. PLE occurs as commonly in women and men, but is less frequent than CLE. It is a characteristic finding in those with homozygous deficiency of serum alpha-1 antitrypsin. It has also been found that certain populations of IV Ritalin abusers show PLE.
Bullae are common in both CLE and PLE, but may exist in the absence of either. Air-filled spaces in the visceral pleura are commonly termed blebs, and those in the parenchyma greater than 1 cm in diameter are called bullae. A valve mechanism in the bronchial communication of a bulla permits air trapping and enlargement of the air space. This scenario may compress the surrounding normal lung. Blebs may rupture into the pleural cavity causing a pneumothorax, and through a valve mechanism in the bronchopleural fistula a tension pneumothorax may develop.
Paracicatricial emphysema occurring adjacent to pulmonary scars represents another type of localized emphysema. When the air spaces distal to terminal bronchioles are increased beyond the normal size but do not show destructive changes of the alveolar walls, the condition is called pulmonary overinflation. This condition may be obstructive, because of air trapping beyond an incomplete bronchial obstruction due to a foreign body or a neoplasm. Many lung lobules may be simultaneously affected as a result of many check-valve obstructions, as in bronchial asthma. Pulmonary overinflation may also be nonobstructive, less properly called “compensatory emphysema”, when associated with atelectasis or resection of other areas of the lung.
Bronchiectasis
Bronchiectasis means irreversible dilation and distortion of the bronchi and bronchioles. Saccular bronchiectasis is the classic advanced form characterized by irregular dilatations and narrowing. The term cystic is used when the dilatations are especially large and numerous. Cystic bronchiectasis can be further classified as fusiform or varicose.
Tubular bronchiectasis is simply the absence of normal bronchial tapering and is usually a manifestation of severe chronic bronchitis rather than of true bronchial wall destruction.
Repeated or prolonged episodes of pneumonitis, inhaled foreign objects or neoplasms have been known to cause bronchiectasis. When the bronchiectatic process involves most or all of the bronchial tree, whether in one or both lungs, it is believed to be genetic or developmental in origin.
Mucoviscidosis, Kartagener’s syndrome (bronchiectasis with dextrocardia and paranasal sinusitis), and agammaglobulinemia are all examples of inherited or developmental diseases associated with bronchiectasis. The term pseudobronchiectasis is applied to cylindrical bronchial widening, which may complicate a pneumonitis but which disappears after a few months. Bronchiectasis is true saccular bronchiectasis but without cough or expectoration. It is located especially in the upper lobes where good dependent drainage is available. A proximal form of bronchiectasis (with normal distal airways) complicates aspergillus mucus plugging.
Advanced bronchiectasis is often accompanied by anastomoses between the bronchial and pulmonary vessels. These cause right-to-left shunts, with resulting hypoxemia, pulmonary hypertension and cor pulmonale.
QUOTE FOR WEDNESDAY:
Ike Skelton (born December 20, 1931) is an American politician who was the U.S. Representative for Missouri’s 4th congressional district from 1977 to 2011)
Part 3 CONGESTIVE HEART FAILURE : Treatment, Complications & Tips
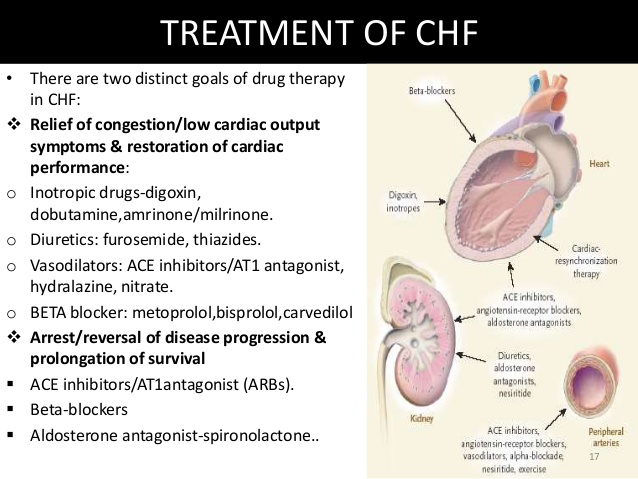
Treatments for CHF:
Heart failure caused by an excessive workload is curable by treating the primary disease, such as anemia or thyrotoxicosis or hypertension or diabetes. Also, curable are forms caused by anatomical problems such as a heart valve defect. These defects can be surgically corrected.
However, for the common forms of heart failure due to damaged heart muscle no known cure (like a heart attack that damages the heart muscle where the attack took place on the organ) but prevention of it happening again can take place in many cases through treatment of the disease or illness with being compliant in following up with your doctor for the disease or illness and being compliant in following doctor’s orders. The worst thing you can do is ignore it. The treatment seeks to improve patients quality of life and length of survival through lifestyle change and drug therapy.
Patients can minimize the effect t of heart failure by controlling the risk factors for heart disease they may have. Obvious steps include: Don’t smoke or quit smoking, lose weight if necessary, abstaining from alcohol, and making those dietary changes to reduce the amount of salt and fat consumed Regular, modest exercise is also helpful for many patinets, though the amount and intensity should be carefully monitored by a physician.
Even with lifestyle changes, most heart failure patients must take medication. Many patients receive 2 or more meds. Types of medication given: ACE inhibitors, Digitalis, Diuretics, Hydralazine, and Nitrates.
These are some of the meds given for heart failure. Not all medications are suitable for patients, and more than one drug may be needed. Always review the list your pharmacist provides in the action, side effects, with instructions of how to take the drug to make it most effective in your body with what to look for while on this medication to keep you the patient most informed on what you should know.
Results of studies over the years have placed more emphasis on the use of drugs known as angiotensin converting enzymes (ACE) inhibitors. Several studies have indicated that ACE inhibitors improve survival among heart failure patients and may slow perhaps even prevent the loss of the heart pumping activity. This drug prevents the transfer of your enzyme Angiotensin 1 to convert to Angiotensin 2 which prevents the vessels in your body to do vasoconstriction which prevents the pressure in the bloodstream to raise = high B/P (hypertension). This prevents stress to the heart, due to high B/this causes blood to get to the heart slowly and more difficult causing the heart to pump harder but the ACE inhibitor with allowing vasodilation (opening of vessels) keeping pressure down to make the job easier= less stress on the heart. Originally these medications where for patients in the treatment of hypertension but they help patients with heart failure, among other things, decreasing the pressure inside the blood vessels causing the heart to do its job easier.
Digitalis increases the force of the heart’s contractions, helping to improve circulation in the body.
Diuretics are for reducing the amount of fluid in the bloodstream and body by releasing them via the kidneys and having us void the excess out in our urine, these are useful for patients with fluid retention.
Those who aren’t prescribed or cannot take these meds already mentioned may be given a hydralazine medication and/or a drug in the Nitrate classification, each of which help relax tension in the blood vessels to improve blood flow. Also, both Hydralazine and Nitrates function is they cause vasodilation in the vessels improving blood flow to the heart.
Sometimes heart failure is life threatening. Usually, this happens when drug therapy and lifestyle changes fail to control its symptoms. In such cases, a heart transplant may be the only treatment option. However, candidates for transplantation often have to wait months or even years before a suitable donor heart is found.
Studies over the years indicate that some transplant candidates improve during this waiting period through drug treatment and other therapy, and can be removed from the transplant list.
Transplant candidates who do not improve sometimes need mechanical pumps, which are attached to the heart. Called left ventricular assist device (LVADs), the machine takes over part or virtually all of the heart’s blood-pumping activity. However, current LVADs are not permanent solutions for heart failure but are considered bridges to transplantation. Worldwide, about 3,500 heart transplants were performed annually. The vast majority of these are performed in the United States (2,000-2,300 annually). Cedars Sinai Medical Center in Los Angeles, California has performed the most heart transplants in the last three consecutive years performing 95 transplants in 2012 alone. About 800,000 people have a Class IV heart defect indicating a new organ. The degrees of CHF are I, II, III and IV. In learning more about CHF with heart transplants (including becoming a candidate for one) go to wwwtransplantexperience.com or even hearttransplant.com.
Another surgical procedure for heart failure that is available in America is cardiomyoplasty. This is a surgical procedure in which healthy muscle from another part of the body is wrapped around the heart to provide support for the failing heart. Most often the latissimus dorsi muscle is used for this purpose. A special pacemaker is implanted to make the skeletal muscle contract. The electrical stimulator icauses the back muscle to contract, pumping the blood from the heart (this allows the heart to do its job more effectively).
Complications of CHF:
Through the Mayo clinic as a reference regarding complications their website stated: “If you have heart failure, your outlook depends on the cause and the severity, your overall health, and other factors such as your age. Complications can include:
- Kidney damage or failure. Heart failure can reduce the blood flow to your kidneys, which can eventually cause kidney failure if left untreated. Kidney damage from heart failure can require dialysis for treatment.
- Heart valve problems. The valves of your heart, which keep blood flowing in the proper direction through your heart, may not function properly if your heart is enlarged, or if the pressure in your heart is very high due to heart failure.
- Liver damage. Heart failure can lead to a buildup of fluid that puts too much pressure on the liver. This fluid backup can lead to scarring, which makes it more difficult for your liver to function properly.
- Stroke. Because blood flow through the heart is slower in heart failure than in a normal heart, it’s more likely you’ll develop blood clots, which can increase your risk of having a stroke.Tips on CHF:Closely follow your doctor’s instructions, being compliant with the instructions and taking your meds.Control your weight in making it easier for your heart, that’s in failure, to function better (less stress).Limit or stop alcohol consumption as your doctor informs you. The best defense against heart failure is PREVENTION! Almost all the cardiac risk factors can be controlled of eliminated (smoking, obese, high cholesterol, high B/P, diabetes).
- Going to the doctor can be stressful but know he is there for you. It is hard to remember everything you want to ask the doctor with everything you hear at your visit. It helps to prepare a list of questions you may have and bring it with you at your appointment to address to the doctor your concerns. In doing this it helps you with your appointment so you can record the answers by listing them on the paper you have. Before you leave the doctor’s office, be sure you understand your condition and its treatment, including any medications your taking this doctor ordered for you with him or her knowing any other medications you may be on through a different doctor to prevent side effects or adverse reactions but if you forget this about the medications there is always your pharmacist you can ask than your M.D. later. With you knowing this information you will see why it is so vital for you doing all these actions or inter- ventions for your disease that the doctor ordered and you’re more out to follow them as well.
- Of course, stop smoking permanently if actively smoking.
- Watch what you eat and how much. Watch the diet intake of cholesterol and sodium that can cause a negative impact on the heart by causing stress to the organ through either high B/P=high sodium that causes vasoconstriction or high cholesterol frequently=blockage in an artery and both cause diminishing of oxygenated blood getting to the heart. Without oxygen to our tissues or cells this causes tissue & cellular starvation. What is starvation to the heart=chest pain (what we call angina). Take a brittle diabetic, the furthest area from the heart is the feet the first area to experience starvation is the toes, foot or lower extremity which is why this is usually the first to be amputated if necessary (you usually see an upper extremity amputated due to trauma).
- Immediately call your doctor of any significant change in your condition, such as an intensified shortness of breath or swollen feet or weight gain of 3lbs or more within one week.
- See your doctor regularly in evaluating your CHF.
- Some people’s symptoms and heart function will improve with proper treatment. However, heart failure can be life-threatening. People with heart failure may have severe symptoms, and some may require heart transplantation or support with an artificial heart device.”
If you are needing any guidance in how to lose weight through using all 4 food groups, with assistance in what to eat now to lose weight till in therapeutic range for your height than eating food from the market or needing to understand how the body works with food and metabolism with where activity comes into play go to healthyusa.tsfl.com and see what we can provide you in answering all these questions for you through Dr. Anderson and myself as your coach free. SO LIVE AS HEALTHY AS POSSIBLE IN YOUR ROUTINE HABITS, YOUR DIETING OF THE 4 FOOD GROUPS, MAINTAINING YOUR WEIGHT IN A THEREPEUTIC RANGE (look as calculating BMI online for free to find out what your weight range for your height is), and BALANCING REST WITH EXERCISE TO HELP DECREASE THE CHANCE OF GETTING HEART FAILURE. Go to healthyusa.tsfl.com to learn what Dr. Anderson through his book of “Dr. A.’s Healthy Habits” and me (for free) as your health coach could provide you with. Just take a view of what can be offered to you for no price with no hacking go to healthyusa.tsfl.com and take a peek;) Join me like many who are trying to live life healthier with making America a healthier home and we all should take part to help the health care system to be more effective for our society. Recommended to anyone with disease before changing your diet, activity/exercise program review with your doctor to get clearance to maintain your safety.