“Keeping Legionella bacteria out of water is the key to preventing infection.”
CDC Centers for disease control and prevention
“Keeping Legionella bacteria out of water is the key to preventing infection.”
CDC Centers for disease control and prevention
“The term “legionellosis” may be referred to either Legionnaires’ disease or Pontiac fever.”
CDC Center for Disease Control
“Legionnaires’ disease (LEE-juh-nares) is caused by a type of bacterium called Legionella (LEE-juh-nell-a). The bacterium is named after a 1976 outbreak, when many people who went to a Philadelphia convention of the American Legion suffered from this disease, a type of pneumonia (lung infection).”
CENTER FOR DISEASE CONTROL
A Baker’s cyst, also called a popliteal (pop-luh-TEE-ul) cyst, is usually the result of a problem with your knee joint, such as arthritis or a cartilage tear.
MAYO CLINIC
“NAFLD affects about 25 percent of the people in the United States, including children. People who are overweight or obese, have high cholesterol and/or triglycerides, or have diabetes, are most likely to contract this liver ailment. Overweight children are being diagnosed more and more frequently with this disease.”
WEB MD
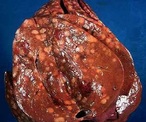
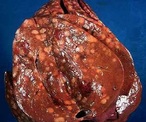 A NASH LIVER (FAT)
A NASH LIVER (FAT)NASH What is NASH?
Nonalcoholic steatohepatitis (NASH) is liver inflammation and damage caused by a buildup of fat in the liver. It is part of a group of conditions called nonalcoholic fatty liver disease. You may be told you have a “fatty liver.” Many people have a buildup of fat in the liver, and for most people it causes no symptoms and no problems. But in some people, the fat causes inflammation and damages cells in the liver. Because of the damage, the liver doesn’t work as well as it should.
There are other conditions like Hemachromatosis (iron overload), which is a metabolic disorder that leads to abnormally elevated amounts of iron that is stored in the body. It is an inherited disease. Wilson’s disease is another inherited disease but it affects the body’s ability to metabolize copper. Gilbert’s Disease is an abnormality in bilirubin metabolism in the liver and affects up to 7% of the North American population.
“The sooner you treat your Hep C, the better your chances may be of being cured, meaning the virus can no longer be detected in your blood.”
Hepatitis C. com
Liver disease is also referred to Hepatic Disease. Liver Disease is a term that is used when there is any disturbance of the liver function that causes illness. It is a broad term to describe when more than 75% or three quarters of liver tissue needed is affected and decreased function in the liver occurs. The number one cause of liver disease is alcohol abuse in North America. They can cause liver inflammation, referred to as alcoholic hepatitis. Other causes include Cirrhosis, Cholestasis, Steatosis, Hepatitis, Viruses, Non-Alcoholic Fatty Liver, Hemachromatosis, Wilson’s Disease and Gilbert’s Disease.
Causes: Cirrhosis
Cirrhosis is when the liver cells are replaced by permanent scar tissue as a result of chronic liver disease. It is considered the late-stage of liver disease. Cirrhosis is common among chronic alcohol abuse users where the fat accumulation occurs in the liver cells and causes scar tissue. Cholestasis is when the bile flow is obstructed from the gallbladder or duodenum. Steatosis is the term used when cholesterol and triglycerides accumulate in the liver.
Causes: Hepatitis
Hepatitis is a term used to describe the inflammation on liver cells. They can become inflamed due to infection.
There are many forms of Hepatitis:
Hepatitis A (Hep A) is a viral infection primarily spread through the fecal-oral route when small amounts of infected fecal matter are ingested. An acute inflammation of the liver occurs but there is a way to prevent this type of infection. There is a vaccine available and the best way to help prevent it is by a good hand washing.
Hepatitis B (Hep B) is spread by exposure to body fluids and can cause an acute infection. If left untreated, it can progress into a chronic inflammation and on into cirrhosis. There is also a vaccine for this form of hepatitis. Typically, the vaccine contains both Hep A and B in a combination series of doses.
Hepatitis C (Hep C) is caused by a virus different from Hep A or Hep B. It can either be “acute” or “chronic” and is primarily spread through contact with the blood of an infected person. The most common way is by sharing needles or other equipment to inject drugs. Before 1992, Hepatitis C was also commonly spread through blood transfusions and organ transplants which led to the start of a widespread screening of blood supplies. Another way it can be transmitted is through being born to a mother who has it. There are less common ways to contract Hepatitis C, and that’s through sharing personal care items that may have come into contact with another person’s blood (razors, toothbrushes), or having unprotected sex with a infected person. Some people are at an increased risk for Hepatitis C. Those individuals include: Children born to mothers infected with this Hep C; current injection drug users (most common way Hepatitis C is spread in the US), past injection drug users, recipients of donated blood (blood products and organs), hemodialysis patients who spent many years on dialysis for kidney failure, people who received body piercings or tattoos done with non-sterile instruments, & people with known exposure to Hepatitis C like Health care workers or recipients of blood or organs from a donor who tested positive.
Hepatitis D (Hep D) is known as “delta hepatitis” can also be “acute” or “chronic” but is uncommon in the United States. It requires the Hepatitis B virus to survive. It is transmitted through sexual contact with infected blood or blood products. There is also no vaccine available for this virus. Hepatitis E (Hep E) is caused by Ribonucleic Acid (RNA) virus. It is transmitted mainly through the fecal-oral route due to fecal contaminated drinking water.
Causes: NAFLD
Non-alcoholic fatty liver disease (NAFLD) is the build up of extra fat in liver cells that is not caused by alcohol. It is normal for the liver to contain some fat. liver’s weight is fat, then it NAFLD tends to develop in people who are overweight or obese or have diabetes, high cholesterol or high triglycerides. Rapid weight loss and poor eating habits also may lead to NAFLD. However, some people develop NAFLD even if they do not have any risk factors. NAFLD affects up to 25% of people in the United States. However, if more than 5% up to 10% of the liver’s weight is fat then the liver is called a fatty liver called steatosis. Non-Alcoholic Fatty Liver (NAFL) describes the accumulation of fat within the liver that can cause an inflammation and a gradual decrease in function.
Those at risk for NAFLD? NAFLD tends to develop in people who are overweight or obese or have diabetes, high cholesterol or high triglycerides. Rapid weight loss and poor eating habits also may lead to NAFLD. However, some people develop NAFLD even if they do not have any risk factors. NAFLD affects up to 25% of people in the United States.
RISKS NAFLD may cause the liver to swell (steatohepatitis). A swollen liver may cause scarring (cirrhosis) over time and may even lead to liver cancer or liver failure.
SYMPTOMS NAFLD often has no symptoms. When symptoms occur, they may include fatigue, weakness, weight loss, loss of appetite, nausea, abdominal pain, spider-like blood vessels, yellowing of the skin and eyes (jaundice), itching, fluid build up and swelling of the legs (edema) and abdomen (ascites), and mental confusion.
DIAGNOSIS NAFLD is initially suspected if blood tests show high levels of liver enzymes. However, other liver diseases are first ruled out through additional tests. Often, an ultrasound is used to confirm the NAFLD diagnosis.
TREATMENT There are no medical treatments yet for NAFLD. Eating a healthy diet and exercising regularly may help prevent liver damage from starting or reverse it in the early stages.


The Liver and its anatomy and physiology:
Weighing in at around 3 pounds, the liver is the body’s second largest organ; only the skin is larger and heavier. The liver performs many essential functions related to digestion, metabolism, immunity, and the storage of nutrients within the body. These functions make the liver a vital organ without which the tissues of the body would quickly die from lack of energy and nutrients. Fortunately, the liver has an incredible capacity for regeneration of dead or damaged tissues.
The liver is a roughly triangular organ that extends across the entire abdominal cavity just inferior to the diaphragm. Most of the liver’s mass is located on the right side of the body where it descends inferiorly toward the right kidney. The liver is made of very soft, pinkish-brown tissues encapsulated by a connective tissue capsule. This capsule is further covered and reinforced by the peritoneum of the abdominal cavity, which protects the liver and holds it in place within the abdomen.
The peritoneum connects the liver in 4 locations: the coronary ligament, the left and right triangular ligaments, and the falciform ligament. These connections are not true ligaments in the anatomical sense; rather, they are condensed regions of peritoneal membrane that support the liver.
The liver has a remarkable capacity to regenerate after injury and to adjust its size to match its host. The liver is an amazing and such a vital organ we need to keep healthy for if we don’t disease comes on. Check out part 2 on liver disease tomorrow.