Breast cancer is cancer that forms in the cells of the breasts.
After skin cancer, breast cancer is the most common cancer diagnosed in women in the United States. Breast cancer can occur in both men and women, but it’s far more common in women.
Public support for breast cancer awareness and research funding has helped improve the diagnosis and treatment of breast cancer. Breast cancer survival rates have increased, and the number of deaths has been declining, thanks to a number of factors such as earlier detection, new treatments and a better understanding of the disease.
Breast Cancer affects everyone. Every year, over 200,000 women are diagnosed with new cases of Breast Cancer in the United States, and over 39,000 women will lose their fight with this terrible disease. Having experienced the effects that cancer has on both the victim and their loved ones support is so important by family and significant ones in our lives.
The Breast Cancer Awareness Month, marked in countries across the world every October, helps to increase attention and support for the awareness, early detection and treatment as well as palliative care of this disease.
There are about 1.38 million new cases and 458 000 deaths from breast cancer each year (IARC Globocan, 2008). Breast cancer is by far the most common cancer in women worldwide, both in the developed and developing countries. In low- and middle-income countries the incidence has been rising up steadily in the last years due to increase in life expectancy, increase urbanization and adoption of western lifestyles.
Currently there is not sufficient knowledge on the causes of breast cancer, therefore, early detection of the disease remains the cornerstone of breast cancer control. When breast cancer is detected early, and if adequate diagnosis and treatment are available, there is a good chance that breast cancer can be cured. If detected late, however, curative treatment is often no longer an option. In such cases, palliative care to relief the suffering of patients and their families is needed.
The majority of deaths (269 000) occur in low- and middle-income countries, where most women with breast cancer are diagnosed in late stages due mainly to lack of awareness on early detection and barriers to health services.
Here is another thing to help breast cancer patients National Breast Cancer Awareness Month is a chance to raise awareness about the importance of early detection of breast cancer. Make a difference! Spread the word about mammograms and encourage communities, organizations, families, and individuals to get involved.
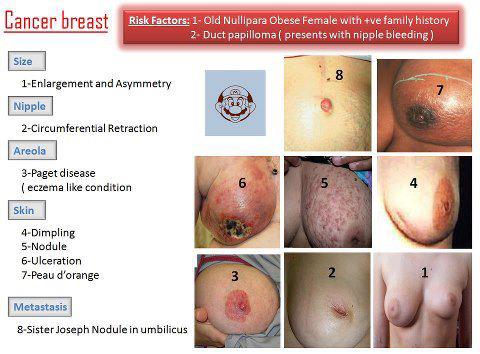
In the first phases, the breast cancer has no evident signs and symptoms and it differ in folks from lumps to swelling and alterations in the pores and skin. A lump also modest which is felt does not cause any strange changes and it is unnoticed. Nevertheless, in a lot of circumstances visual appeal of new lump or a mass is the 1st indicator discovered. The lump may possibly be difficult to contact with uneven edges and they are painless. But there are cases the lump is really tender, spherical edged and soft. More lumps are painless. Breast Most cancers Signs and symptoms are: Swelling of element of the breast or all areas Pores and skin irritation in the breast. Nipple pain, Nipple begins to switch inward (inverted) slowly and gradually Breast pain.
Breast cancer prevention starts with healthy habits — such as limiting alcohol and staying physically active. Understand what you can do to reduce your breast cancer risk.
If you’re concerned about breast cancer, you may be wondering if there are steps you can take toward breast cancer prevention. Some risk factors, such as family history, can’t be changed. However, there are lifestyle changes you can make to lower your risk.
What can I do to reduce my risk of breast cancer?
Lifestyle changes have been shown in studies to decrease breast cancer risk even in high-risk women. The following are steps you can take to lower your risk:
- Limit alcohol. The more alcohol you drink, the greater your risk of developing breast cancer. If you choose to drink alcohol — including beer, wine or liquor — limit yourself to no more than one drink a day.
- Don’t smoke. Accumulating evidence suggests a link between smoking and breast cancer risk, particularly in premenopausal women. In addition, not smoking is one of the best things you can do for your overall health.
- Control your weight. Being overweight or obese increases the risk of breast cancer. This is especially true if obesity occurs later in life, particularly after menopause.
- Be physically active. Physical activity can help you maintain a healthy weight, which, in turn, helps prevent breast cancer. For most healthy adults, the Department of Health and Human Services recommends at least 150 minutes a week of moderate aerobic activity or 75 minutes of vigorous aerobic activity weekly, plus strength training at least twice a week.
- Breast-feed. Breast-feeding may play a role in breast cancer prevention. The longer you breast-feed, the greater the protective effect.
- Limit dose and duration of hormone therapy. Combination hormone therapy for more than three to five years increases the risk of breast cancer. If you’re taking hormone therapy for menopausal symptoms, ask your doctor about other options. You may be able to manage your symptoms with nonhormonal therapies, such as physical activity. If you decide that the benefits of short-term hormone therapy outweigh the risks, use the lowest dose that works for you.
- Avoid exposure to radiation and environmental pollution. Medical-imaging methods, such as computerized tomography, use high doses of radiation, which have been linked with breast cancer risk. Reduce your exposure by having such tests only when absolutely necessary. While more studies are needed, some research suggests a link between breast cancer and exposure to the chemicals found in some workplaces, gasoline fumes and vehicle exhaust. Eating a diet rich in fruits and vegetables hasn’t been consistently shown to offer protection from breast cancer. In addition, a low-fat diet appears to offer only a slight reduction in the risk of breast cancer.
- However, eating a healthy diet may decrease your risk of other types of cancer, as well as diabetes, heart disease and stroke. A healthy diet can also help you maintain a healthy weight — a key factor in breast cancer prevention.
- Can a healthy diet prevent breast cancer?
Stay tune for Part II tomorrow on breast cancer.