I went to several different grade schools all over the West Coast. I got polio when I was 8 and spent eight months in the hospital and a rehab clinic in Seattle.
Dennis Washington
I went to several different grade schools all over the West Coast. I got polio when I was 8 and spent eight months in the hospital and a rehab clinic in Seattle.
Dennis Washington


Around 40% of people who survive paralytic polio may develop additional symptoms 15–40 years after the original illness. These symptoms – called post-polio syndrome – include new progressive muscle weakness, severe fatigue and pain in the muscles and joints.
Around 40% of people who survive paralytic polio may develop additional symptoms 15–40 years after the original illness. These symptoms – called post-polio syndrome – include new progressive muscle weakness, severe fatigue and pain in the muscles and joints.
Post-polio syndrome is an illness of the nervous system that can appear 15 to 50 years after you had polio. It affects your muscles and nerves, and it causes you to have weakness, fatigue, and muscle or joint pain.
Although post-polio syndrome can make some day-to-day activities more difficult, treatment can help control symptoms and help you stay active. Your symptoms may not get worse for many years. Post-polio syndrome usually progresses very slowly.
Post-polio syndrome most likely arises from the damage left over from having the polio viruse in the body still.
The polio virus harms the nerves that control muscles, and it makes the muscles weak. If you had polio, you may have gained back the use of your muscles. But the nerves that connect to the muscles could be damaged without your knowing it. The nerves may break down over time and cause you to have weak muscles again.
Symptoms of post-polio syndrome tend to show up very slowly. The main symptoms are:
Depending on which muscles are affected, this trio of muscle weakness, fatigue, and pain can make daily activities more difficult. For example, people with shoulder or arm weakness may have trouble getting dressed. People who have weakness in their legs may have trouble walking or climbing stairs.
Post-polio syndrome is rarely life-threatening, but the symptoms can significantly interfere with an individual’s ability to function independently. Respiratory muscle weakness, for instance, can result in trouble with proper breathing, affecting daytime functions and sleep. Weakness in swallowing muscles can result in aspiration of food and liquids into the lungs and lead to pneumonia.
Only a polio survivor can develop PPS.
The severity of weakness and disability after recovery from poliomyelitis tends to predict the relative risk of developing PPS. Individuals who had minimal symptoms from the original illness are more likely to experience only mild PPS symptoms. A person who was more acutely affected by the polio virus and who attained a greater recovery may experience a more severe case of PPS, with greater loss of muscle function and more severe fatigue.
The exact incidence and prevalence of PPS is unknown. The U.S. National Health Interview Survey in 1987 contained specific questions for persons given the diagnosis of poliomyelitis with or without paralysis. No survey since then has addressed the question. Results published in 1994-1995 estimated there were about 1 million polio survivors in the U.S., with 443,000 reporting to have had paralytic polio. Accurate statistics do not exist today, as a percentage of polio survivors have died and new cases have been diagnosed. Researchers estimate that the condition affects 25 to 40 percent of polio survivors.
The cause of PPS is unknown but experts have offered several theories to explain the phenomenon—ranging from the fatigue of overworked nerve cells to possible brain damage from a viral infection to a combination of mechanisms. The new weakness of PPS appears to be related to the degeneration of individual nerve terminals in the motor units. A motor unit is formed by a nerve cell (or motor neuron) in the spinal cord or brain stem and the muscle fibers it activates. The polio virus attacks specific neurons in the brain stem and spinal cord. In an effort to compensate for the loss of these motor neurons, surviving cells sprout new nerve-end terminals and connect with other muscle fibers. These new connections may result in recovery of movement and gradual gain in power in the affected limbs. Years of high use of these recovered but overly extended motor units adds stress to the motor neurons, which over time lose the ability to maintain the increased work demands. This results in the slow deterioration of the neurons, which leads to loss of muscle strength. Restoration of nerve function may occur in some fibers a second time, but eventually nerve terminals malfunction and permanent weakness occurs. This hypothesis explains why PPS occurs after a delay and has a slow and progressive course.
Through years of studies, scientists at the National Institute of Neurological Disorders and Stroke (NINDS) and at other institutions have shown that the weakness of PPS progresses very slowly. It is marked by periods of relative stability, interspersed with periods of decline.
The diagnosis of PPS relies nearly entirely on clinical information. There are no laboratory tests specific for this condition and symptoms vary greatly among individuals. Physicians diagnose PPS after completing a comprehensive medical history and physical examination, and by excluding other disorders that could explain the symptoms.
Physicians look for the following criteria when diagnosing PPS:
PPS may be difficult to diagnose in some people because other medical conditions can complicate the evaluation. Depression, for example, is associated with fatigue and can be misinterpreted as PPS. A number of conditions may cause problems in persons with polio that are not due to additional loss of motor neuron function. For example, shoulder osteoarthritis from walking with crutches, a chronic rotator cuff tear leading to pain and disuse weakness, or progressive scoliosis causing breathing insufficiency can occur years after polio but are not indicators of PPS.
Polio survivors with new symptoms resembling PPS should consider seeking treatment from a physician trained in neuromuscular disorders. It is important to clearly establish the origin and potential causes for declining strength and to assess progression of weakness not explained by other health problems. Magnetic resonance imaging (MRI) and computed tomography (CT) of the spinal cord, electrophysiological studies, and other tests are frequently used to investigate the course of decline in muscle strength and exclude other diseases that could be causing or contributing to the new progressive symptoms. A muscle biopsy or a spinal fluid analysis can be used to exclude other, possibly treatable, conditions that mimic PPS. Polio survivors may acquire other illnesses and should always have regular check-ups and preventive diagnostic tests. However, there is no diagnostic test for PPS, nor is there one that can identify which polio survivors are at greatest risk.
There are currently no effective pharmaceutical treatments that can stop deterioration or reverse the deficits caused by the syndrome itself. However, a number of controlled studies have demonstrated that non-fatiguing exercises may improve muscle strength and reduce tiredness. Most of the clinical trials in PPS have focused on finding safe therapies that could reduce symptoms and improve quality of life.
Researchers at the National Institutes of Health (NIH) have tried treating persons having PPS with high doses of the steroid prednisone and demonstrated a mild improvement in their condition, but the results were not statistically significant. Also, the side effects from the treatment outweighed benefits, leading researchers to conclude that prednisone should not be used to treat PPS.
Preliminary studies indicate that intravenous immunoglobulin may reduce pain and increase quality of life in post-polio survivors.
A small trial to treat fatigue using lamotrigine (an anticonvulsant drug) showed modest effect but this study was limited and larger, more controlled studies with the drug were not conducted to validate the findings.
Although there are no effective treatments, there are recommended management strategies. Patients should consider seeking medical advice from a physician experienced in treating neuromuscular disorders. Patients should also consider judicious use of exercise, preferably under the supervision of an experienced health professional. Physicians often advise patients on the use of mobility aids, ventilation equipment, revising activities of daily living activities to avoid rapid muscle tiring and total body exhaustion, and avoiding activities that cause pain or fatigue lasting more than 10 minutes. Most importantly, patients should avoid the temptation to attribute all signs and symptoms to prior polio, thereby missing out on important treatments for concurrent conditions. Always go to your physician for advisement before starting any exercise regimen to make sure your M.D. clears the activity first, for your safety!
Victor Davis Hanson (born September 5, 1953) is an American military historian, columnist, former classic professor, and scholar of ancient warfare
Bryan Adams (born 5 November 1959) is a Canadian rock singer-songwriter, musician, producer, actor and photographer. Best known for hit singles including “Summer of ’69“, “Run To You“, number one single “Everything I Do (I Do It For You)” and “18 Til I Die“.

What is diabetes?
Diabetes is a group of diseases marked by high levels of blood glucose resulting from defects in insulin production, insulin action, or both. Diabetes can lead to serious complications and premature death, but people with diabetes, working together with their support network and their health care providers, can take steps to control the disease and lower the risk of complications.
There are 2 types:
Type 1 diabetes was previously called insulin-dependent mellitus (IDDM) or juvenile-onset diabetes. This type of diabetes happens when the immune system ends up destroying beta cells in the body that come from our pancreas and they are the only cells in the human body that make the hormone INSULIN the regulates your glucose. Insulin allows glucose to transfer into the cells and tissues of our body to give them their energy to do their job in the body and nutrition to work properly=sugar-glucose. To live with this diabetes the person must have their insulin delivered by injection or a pump. This form of diabetes usually occurs in children or young adults but can occur at any age.
Type 2 diabetes was called non-insulin dependent diabetes mellitus (NIDDM) or adult-onset diabetes. In adults, type 2 diabetes accounts for about 90-95% of all diagnosed cases of diabetes. It usually begins as insulin resistance, a disease in which the cells do not use insulin properly due to the pancreas not making enough or the pancreas not secreting the correct form o of insulin to do its function. Ending line the insulin isn’t working properly. As the need for insulin rises, the pancreas gradually loses its ability to produce it.
Type 2 diabetes is associated with older age, OBESITY, family history of diabetes, history of gestational diabetes, impaired glucose metabolism, physical inactivity and race/ethnicity.
Gestational diabetes is a form of glucose intolerance diagnosed during pregnancy. Gestational diabetes occurs more frequently among African Americans, Hispanic/Latino Americans, and American Indians. It is also more common among obese women and women with a family history of diabetes. During pregnancy, gestational diabetes requires treatment to optimize maternal blood glucose levels to lessen the risk of complications in the infant.
Other types of diabetes result from specific genetic conditions (such as maturity-onset diabetes of youth), surgery, medications, infections, pancreatic disease, and other illnesses. Such types of diabetes account for 1% to 5% of all diagnosed cases.
Treating diabetes
Diet, insulin, and oral medication to lower blood glucose levels are the foundation of diabetes treatment and management. Patient education and self-care practices are also important aspects of disease management that help people with diabetes lead normal lives.
Self-management education or training is a key step in improving health outcomes and quality of life. It focuses on self-care behaviors, such as healthy eating, being active, and monitoring blood sugar.
Criteria for the diagnosis of diabetes:
Diabetes is not only common and serious; it is also VERY COSTLY! Let us take a look:
The cost of treating diabetes is staggering. According to the American Diabetes Association, the annual cost of diabetes in medical expenses and lost productivity rose for $98 billion in 1997 to $132 billion in $2002 to $174 billion in 2007.
One out of every 5 U.S. federal health care dollars is spent treating people with diabetes. The average yearly health care costs for a person without diabetes is 2,560 dollars; for a person with diabetes that figure soars to $11,744. Much of the human and financial costs can be avoided with proven diabetes prevention and management steps.
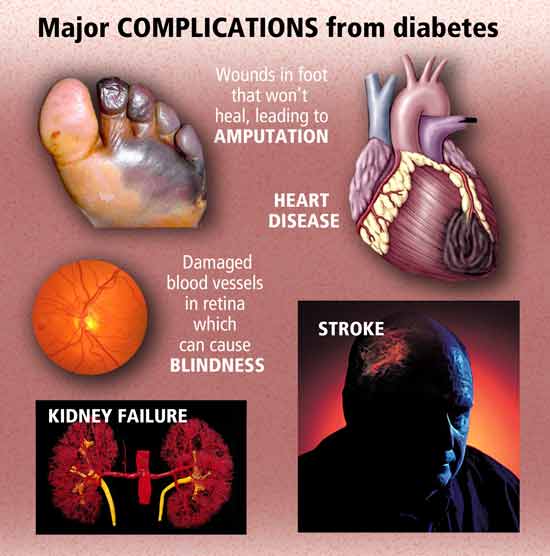
Turn into PART 2 tomorrow and learn what the symptoms and complications are of Diabetes with how to decrease your odds of getting Diabetes with knowing what measures to take to better control your Diabetes, with your doctor’s approval.
REFERENCES for Part 1 and Part 2 :
4.) NIDDK “National Institute of Diabetes and Digestive and Kidney Diseases”
5)National Diabetes Information Clearinghouse (NIDC) – U.S. Department of Health and
Human Services. “Preventing Diabetes Problems: What you need to know”
“Injuries occur from spending too much time in cold, but not freezing, temperatures. The skin does not actually freeze.”
Web M.D
“Some exposure to low temperatures can help activate “brown fat,” which produces heat and burns calories, according to research cited by Harvard Medical School.”
CNN
Go to striveforgoodhealth.com and learn about how cold can be good for your health.
“I was eating bad stuff. Lots of sugar and carbs, junk food all the time. It makes you very irritated.”
Avril Lavigne (31 y/o who is a Canadian singer-songwriter and actress.)
“If you suspect that someone has had a brain injury, the first step is to talk with the person, share your observations, and encourage the person to get help. The next step is for the person to share a medical, family and military history with the physician.”
Harvey E. Jacobs, Ph.D. and Flora Hammond, M.D.
“Civilization, the orderly world in which we live, is frail. We are skating on thin ice. There is a fear of a collective disaster. Terrorism, genocide, flu, tsunamis.”
Zygmunt Bauman (87 y/o and born 19 November 1925 is a Polish sociologist. Since 1971, he has resided in England after being driven out of Poland by ananti-Semetic.)