What are the parts of the nervous system?
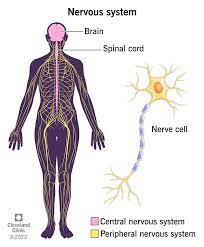
The nervous system has two main parts:
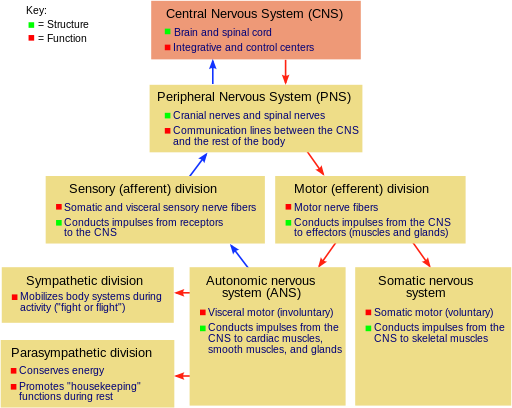
1 – Central nervous system (CNS): Your brain and spinal cord make up your CNS. Your brain reads signals from your nerves to regulate how you think, move and feel.
2 – Peripheral nervous system (PNS): Your PNS is made up of a network of nerves. The nerves branch out from your spinal cord. This system relays information from your brain and spinal cord to your organs, arms, legs, fingers and toes.
Your peripheral nervous system (PNS) is that part of your nervous system that lies outside your brain and spinal cord. It plays key role in both sending information from different areas of your body back to your brain, as well as carrying out commands from your brain to various parts of your body.
Some of those signals, like the ones to your heart and gut, are automatic. Others, like the ones that control movement, are under your control.
What’s the difference between the peripheral and central nervous systems?
Your nervous system consists of two main parts: your central nervous system and your peripheral nervous system.
Your central nervous system includes two organs, your brain and spinal cord.
Your peripheral nervous system is everything else and includes nerves that travel from your spinal cord and brain to supply your face and the rest of your body. The term “peripheral” is from the Greek word that means around or outside the center.
There are two parts to your peripheral nervous system:
- The somatic nervous system guides your voluntary movements.
Your somatic nervous system is a subdivision of your peripheral nervous system, which is all of your nervous system except your brain and spinal cord. Your somatic nervous system allows you to move and control muscles throughout your body. It also feeds information from four of your senses — smell, sound, taste and touch — into your brain.
- The autonomic nervous system regulates the activities you do without thinking about them (involuntary movements).
Your autonomic nervous system is a network of nerves throughout your body that control unconscious processes. These are things that happen without you thinking about them, such as breathing and your heart beating. Your autonomic nervous system is always active, even when you’re asleep, and it’s key to your continued survival.
Your autonomic nervous system is a part of your overall nervous system that controls the automatic functions of your body that you need to survive. These are processes you don’t think about and that your brain manages while you’re awake or asleep.
What does the nervous system look like?
Nerve cells (neurons) are the basis of your nervous system. There are 100 billion neurons in your brain. These cells connect throughout your entire body.
Imagine your nervous system as a tree. Your central nervous system is the trunk of the tree that contains your brain and spinal cord. The tree branches are your peripheral nervous system (nerves). The branches extend from the truck (brain and spinal cord) to reach all parts of your body.
Signs and symptoms of nervous system conditions vary by type but may include:
- Movement and coordination changes.
- Memory loss.
- Pain, numbness or a pins and needles feeling.
- Behavioral and mood changes.
- Difficulty with thinking and reasoning.
- Seizures.
Some conditions, like a stroke, are medical emergencies that need treatment quickly. If you notice the following symptoms, contact 911 or your local emergency services number:
- Muscle weakness or paralysis in one side of your body.
- Sudden vision loss.
- Slurred speech.
- Confusion.