
 10Years Ago
10Years AgoLets see the facts Ebola:
First signs / symptoms range from
- Fever (greater than 38.6°C or 101.5°F)
- Severe headache
- Muscle pain
- Weakness
- Diarrhea
- Vomiting
- Abdominal (stomach) pain
- Unexplained hemorrhage (bleeding or bruising)
Symptoms may appear anywhere from 2 to 21 days after exposure to Ebola, but the average is 8 to 10 days.
Recovery from Ebola depends on good supportive clinical care and the patient’s immune response. People who recover from Ebola infection develop antibodies that last for at least 10 years.
Reference on symptoms of Eboli: (http://www.cdc.gov/vhf/ebola/symptoms/index.html).
Healthcare workers who may be exposed to people with Ebola should follow these steps:
- Wear protective clothing, including masks, gloves, gowns, and eye protection.
- Practice proper infection control and sterilization measures. For more information, see “Infection Control for Viral Hemorrhagic Fevers in the African Health Care Setting”.
- Isolate patients with Ebola from other patients.
- Avoid direct contact with the bodies of people who have died from Ebola.
- Notify health officials if you have had direct contact with the blood or body fluids, such as but not limited to, feces, saliva, urine, vomit, and semen of a person who is sick with Ebola. The virus can enter the body through broken skin or unprotected mucous membranes in, for example, the eyes, nose, or mouth.
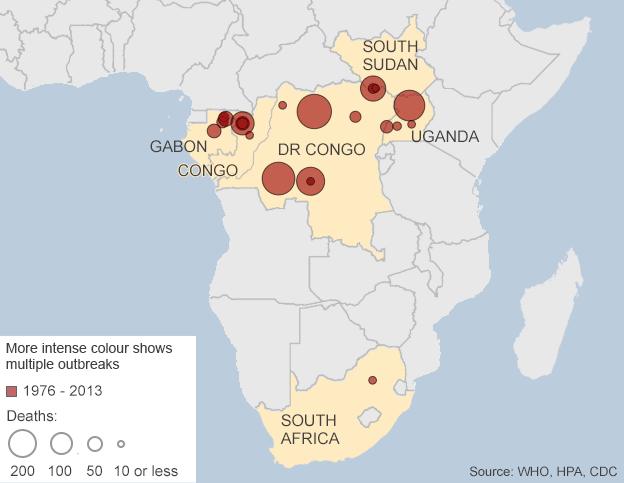
Looking at some of the history is as follows:
In 1995, an outbreak of Ebola hemorrhagic fever (Ebola HF) affected more than 300 people in and around the city of Kikwit, Democratic Republic of the Congo (formerly, Zaire); approximately 80% of the patients died. More than one-fourth of all the patients were health care workers. After the outbreak, the DRC Ministry of Health, the Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) developed practical recommendations for carrying out viral hemorrhagic fever (VHF) isolation precautions in rural health facilities in Africa. These recommendations have been consolidated in a manual for the local health community but something needs to be put into play in getting this epidemic under control if not history noted for repeating itself would be a shame in see results like the following:
The Black Death, 1918 Spanish Flu, HIV/AIDS (As of 2011 at least 60 million people had been infected by AIDS and 25 million had died. while in 2008 an estimated 1.2 million Americans had HIV, Sub-Saharan Africa alone was home to 22.9 million cases, with one in five adults infected. About 35.3 million people were believed to have HIV in 2012.), The Plague of Justinian (ultimately killed 25 million people dead), The Antonine Plague, Cholera, reference to this information is at http://www.rwjf.org/en/blogs/new-public-health/2013/12/the_five_deadliesto.html to go further into details about them.
Other epidemics are Polio, Typhus (camp fever), Malaria, Small Pox, Yellow Fever, The Flu in 1918 before the vaccine. The flu only survived for a year, this strain of virus was responsible for the deaths of 50 to 100 million people, as it was able to quickly spread from country to country as troops and soldiers returned home from WWI from all around the globe. Symptoms were common to those in today’s influenza virus. Also the death for many was the complication of the flu in causing fluid build up in the lungs causing the death (from probably putting the pt into the complication septicemia or or those with or without congestive heart failure going into a exacerbation without having effectively removing the fluids by getting better and ending result drowning in their own lungs).
This is not a pretty picture in having to repeat in history for some Epidemic to occur in our time; which could be Ebola.
Although there is still a great deal to learn about Ebola HF, two observations from the Kikwit outbreak strongly indicate that future outbreaks of this magnitude could be prevented:
- The first case occurred in January 1995, but went unrecognized as Ebola HF by health-care workers. This one case started a chain of transmission of the virus that finally was recognized in April of that year, when many more cases appeared. The outbreak peaked in May. Thus, between January and April, there was a window of opportunity that could have allowed early detection and proper management of patients; the early response might have prevented widespread transmission of the virus.
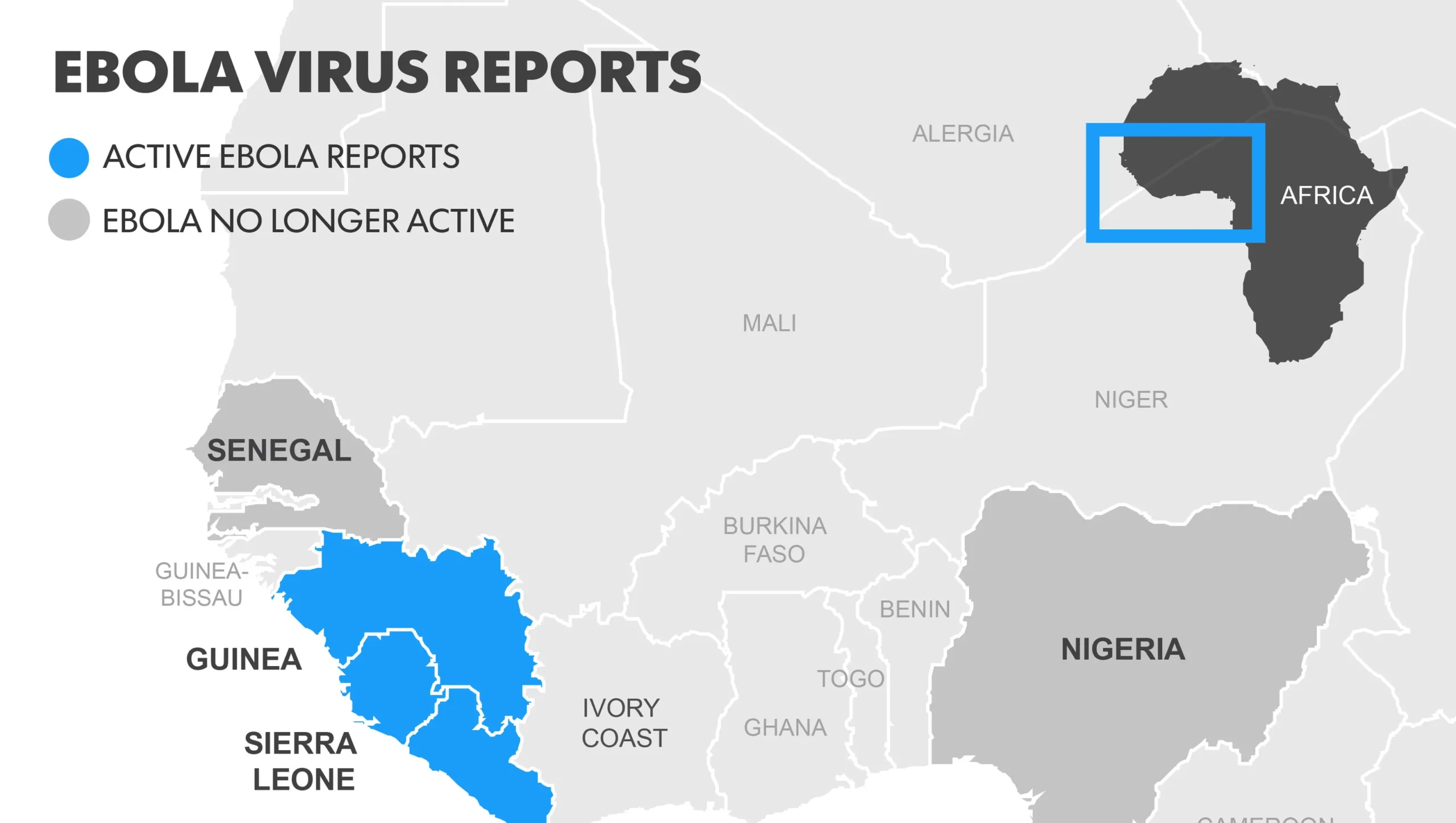
- After an international investigation team arrived in May 1995 and worked with Kikwit medical community to introduce VHF isolation precautions as well as standard precautions, no further nosocomial transmission of the virus was documented, indicating that although Ebola HF is highly infectious, the use of these measures is effective in preventing the spread of disease. Questionable by many since we have it in our country starting an epidemic and it is already an active one in Africa now.
- The observations sent a strong message to the public health and medical communities in Africa and internationally: combining early suspicion of VHF and isolation precautions can help to prevent another serious outbreak of Ebola HF or other VHF in the future. The only question remaining was how these goals could be achieved in a region where resources are scarce and the health care infrastructure is either underdeveloped or deteriorating. This manual, prepared collaboratively by CDC and WHO, attempts to address the issues of early provisional diagnosis and response within a limited infrastructure. It is designed for the following uses: For prevention through preparedness–to help African health facilities make advance preparations for responding with appropriate precautions when a VHF case is suspect.
- For planning and conducting in-service training to strengthen standard precautions and VHF isolation precautions. With follow up by superiors of the facility, from floor managers to nursing education depts.
- As a rapid reference when a VHF case appears at a health facility where no previous VHF preparations have been made give the following by CDC: The recommendations in the manual make use of common, low-cost supplies, such as household bleach, water, cotton cloth, and plastic sheeting. Step-by-step instructions for implementing the recommendations are presented along with instructional aids for easy reference in health centers. For further information on this go to http://www.cdc.gov/vhf/abroad/vhf-manual.html.
- God willing this becomes no epidemic in our country with our government taking better and stronger actions in prevention of diseases spreading in this country. In carrying out stricter rules and regulations which should have been laid down awhile ago regarding people living here or just visiting that travel to and from different countries. This is should have taken place already just by looking at our history of epidemics that have occurred from spread diseases that came some other than United States.