“God often uses desperate moments to wake us up. Only when things start to fall apart do we finally open our eyes.”
― Kyle Idleman, AHA: The God Moment That Changes Everything
Part II Signs and Symptoms with Diagnosing of CHF.
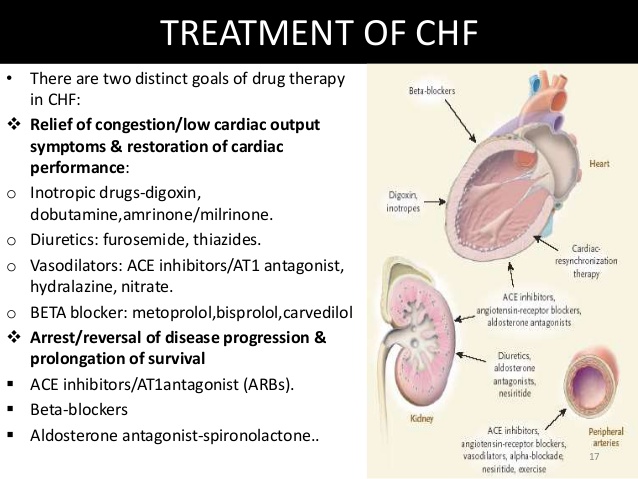
Part 2 Congestive Heart Failure:Signs & Symptoms and diagnosing.
Heart failure can be ongoing (chronic), or your condition may start suddenly (acute).
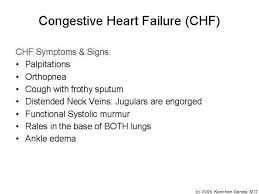
Heart failure signs and symptoms may include:
- Shortness of breath (dyspnea) when you exert yourself or when you lie down
- Fatigue and weakness
- Swelling (edema) in your legs, ankles and feet
- Rapid or irregular heartbeat
- Reduced ability to exercise
- Persistent cough or wheezing with white or pink blood-tinged phlegm
- Increased need to urinate at night
- Swelling of your abdomen (ascites)
- Sudden weight gain from fluid retention
- Lack of appetite and nausea
- Difficulty concentrating or decreased alertness
- Sudden, severe shortness of breath and coughing up pink, foamy mucus
- Chest pain if your heart failure is caused by a heart attack
- To diagnose heart failure, your doctor will first ask you questions about your medical symptoms and history. Your doctor will want to know:
- if you have any other health conditions such as diabetes, kidney disease, angina, high blood pressure, or other heart problems.
- if you smoke
- if you drink alcohol and how much you drink
- what medications you are taking
- Your doctor will also perform a complete physical exam. Your doctor will look for signs of heart failure as well as any other illnesses that may have caused your heart to weaken.
QUOTE FOR WEDNESDAY:
I saw many people who had advanced heart disease and I was so frustrated because I knew if they just knew how to do the right thing, simple lifestyle and diet steps, that the entire trajectory of their life and health would have been different.
Mehmet Oz (born June 11, 1960), better known as Dr. Oz, is a Turkish – American cardiothoracic surgeon, author, and television personality.
QUOTE FOR TUESDAY:
“The law of the heart is thus the same as the law of muscular tissue generally, that the energy of contraction, however measured, is a function of the length of the muscle fibre. ”
— Ernest Henry Starling (17 April 1866 – 2 May 1927 He was an English physiologist. He worked mainly at University College London, although he also worked for many years in Germany and France.
The HEART is the ENGINE of the body!

Let us first understand how the heart functions. For starters think of a car, without the engine the car won’t move unless pushed in neutral but the engine is still not working at all. Well, the body can’t work at all if the heart isn’t working=dead. Right? We can’t live without the heart but more importantly you can’t function actively and productively with a one that is diseased not cared for or just severely diseased. We need to take good care of our bodies especially if diseased already, that includes your heart.
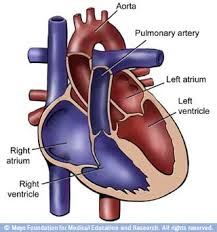
Looking at the anatomy and physiology of the heart it will help us understand in how it functions. For starters the heart is like the engine of the human body based on its characteristics in that without it we would not be able to function or live; just like a car would not function without an engine. The heart’s anatomy let us start with. In the heart you have chambers (2 on the top called atriums and 2 on the bottom called ventricles), 4 chambers to be exact (sort of like a 4 cylinder car). It also has valves which allows our blood to go in and out of the chambers and vessels of the heart. That is what makes blood move throughout the circulatory system starting from the heart down the abdomen to the arms, than the legs/feet back up to the brain to the heart again. These valves are located before the entrance of the blood entering the heart on right upper chamber, between the upper and lower chambers (atriums & ventricles), at the beginning of arteries and veins involved in moving blood throughout the heart and to or from the lungs to exchange oxygen and carbon dioxide from and into the blood. Lastly, in our veins the legs have valves to push blood back up to the heart because this blood that had high oxygen cells are not filled with more carbon dioxide. When this blood is pushed up in the legs through the veins by valves allowing the blood to return to the heart with more carbon dioxide in the blood this is done to allow that blood to get to the lungs for oxygen and carbon dioxide to transfer (like oil/gas entering the car first in the tank and used throughout the engine and leaves the muffler out the tail pipe (the car’s lungs). Oxygen is our gas to the body without it we couldn’t survive but to get it we have to breath to allow oxygen and carbon dioxide to go in and out of our cells at the bases of the lungs where the blood cells pass by in the circulatory system for the transfer of 02 and CO2 to take place. For this to take place it is when we breath; which is allowing 02 in the body and carbon dioxide (used up oxygen in that cell) to be released from the cell and removed through the lungs on expiration.
Now getting down in how the heart works. First take our blood, in particular our red blood cells are the cells that carry oxygen and carbon dioxide throughout our body; the body without enough oxygen in the body tissues=cellular starvation. We can’t survive without oxygen sent to our tissues=food to our tissues (Ex. poor circulation to any tissue of the body = pain and if not resolved it will go into necrosis = death of the tissue, like in a diabetic that has poor circulation to the toes/foot that has pain/numbness and unresolved = necrosis to amputation). So your blood, in particular the red blood cells, need to transport oxygen (O2) to and take carbon dioxide (CO2) from our tissues in the body and refill up with more 02 and release C02 (O2 used up by our tissues) which takes place at the lungs. This process is done constantly in the body to feed our tissues O2 (by the red blood cells-RBC’s picking up 02 upon inhalation) with tissues releasing CO2 which is picked up by the RBC’s and they take the CO2 to the lungs in releasing it from our body completely via exhaling. This whole process is only done due to the heart beating allowing the blood to circulate and recirculate throughout the body and get more 02 from our lungs (just like the engine of a car in how the engine works to allow fuels, oils to circulate throughout the engine and other areas of the car to allow the car overall to function but when the gas gets low we refill it up at the gas station with more car gas).
In review, our bodies oxygen is the food to our tissues in keeping them alive through our red blood cells (RBC’s) that carry the O2 to the tissues through a working heart and lungs only (one organ cannot live without the other). There has to be a systemic way we allow this to work and this is through the heart, lungs, and RBC’s (3 systems that connect with each other). The heart = right side deals with more C02 blood which is blood returning to the heart to get more 02 going first via the Rt. side of the heart to the Rt. and Lt. pulmonary artery, each of which carries blood to the lungs for 02 and C02 exchange to occur. This is for getting more 02 in our RBC’s with allowing them to release C02 at the lungs and then return them to the left side of the heart to be sent through both Lt. chambers of the heart to our blood stream to utilize the new 02 in our RBC’s to our body tissues. This is a 24hr/7days a week job for our red blood cells, lungs and heart in functioning to keep the human body alive.
In simpler terms this is how it works: The blood that needs to be refreshed with more 02 always enters the right (Rt.) atrium coming from a vessel that brings back mainly carbon dioxide in the blood from the toes and the brain that was mainly used up by the tissues and those RBC’s need to be reoxygenated with higher levels of oxygen for the RBC’s to deliver 02 again to tissues. It first goes to the Rt. atrium & fills up to its max level simultaneously while the left (Lt.) atrium is filling up to its max level. When the Rt. atrium is ready to drop its blood max level into the Rt. ventricle below it the valves open between the chambers simultaneously (the tricuspid valve and mitral valve) dropping the blood to the Rt. Ventricle (Lt side does the same thing) but only the Rt. side ends up going to the lungs through a Rt. and Lt. pulmonary artery to get more oxygen to send the highly oxygenated blood to the L (left) side of the heart. The job the Rt. side of the heart does is this, it just goes from the Rt. side of the heart to our lungs and back to the heart on the Lt. side through the 4 pulmonary veins to the L atrium; so the path or distance for the Rt. side of the heart to do its function is a short distance = it gets your used up oxygen in the red blood cells (that are high in carbon dioxide) to get more oxygen by going through the Rt. side of the heart sending them to the lungs where they get more O2 and then they are sent back to the Lt. side of the heart. This is the Rt. side of the heart’s function and explains why the heart muscle on that side of the heart is smaller than the Lt. side. Now let us look at what the Lt. side of the heart in what it does in its function. The RBC’s reoxygenated that leave the lungs and are sent via the pulmonary vein to the Lt. side of the heart, reaching the Lt. atrium, thus carries a high 02 level in the RBC’s (this blood just came directly from the lungs where O2 and CO2 exchange for the RBC’s took place).
Next the RBC’s go to the Lt. ventricle to our Aorta that sends this high oxygen level of RBC’s out to all our tissues as food to prevent starvation of the tissues. Again, when the valves open between the chambers and allowing this blood to fill up in the lower chambers called the Rt. and Lt. ventricles it is simultaneously done also including the valves that open and close in the heart the pulmonary artery and the aorta that is in the Rt and Lt. The ventricle sending RBC’s out to our circulatory system high in O2 to be utilized by our body tissues is the Lt. Ventrilcle. To do this job takes more effort as opposed to the Rt. Side of the heart and that is why the Lt side of the heart has a bigger muscle mass (more of a work out for the heart).
So the way it works with both sides of the heart is the Rt. side sends blood of highly carbon dioxide blood (RBC’s) to the lungs to get re-oxygenated through 2 vessels from the Rt. side of the heart to the lungs that sends this re-oxygenated blood in the RBC’s through 4 vessels to the Lt. side of the heart and it reaches the Lt. side of the heart which sends this highly oxygenated blood throughout the top and bottom of the Lt. side of the heart to the aorta that sends this blood throughout our body tissues. When this oxygen is used all up from the RBC’s dispensing it out to tissues the C02 is taken back from the tissues by RBC’s that replace it with O2 through breathing, this process starts all over again with these RBC’s that returned to the heart. Ending line the right side of the heart is for higher levels of carbon dioxide in the blood (used up blood) to get more oxygen whereas the left side of the heart sends higher levels of O2 throughout the body all the way to the toes (a harder job=muscle mass of the left side of the heart works out more than the right making the left side of the heart a bigger muscle vs the right side).
Now knowing the anatomy and physiology of the heart let’s now understand more about a cardiac disease RVR=Rapid Ventricular Rate and Atrial Fibrillation and more regarding how they develop and in how it effects the engine of the body, being the heart, and the lungs, the transmission of the body. Like a car if the engine is affected in time the transmission gets affected and if not repaired by the mechanic the car engine will die with the transmission. Same effect with the human engine=the heart. If the heart is affected in time it will effect the lungs and if not repaired the heart will die and so will the lungs.
QUOTE FOR MONDAY:
“Our mothers, daughters, sisters and friends are at risk. Heart disease and stroke cause 1 in 3 deaths among women each year – more than all cancers combined. Fortunately, we can change that because 80 percent of cardiac events can be prevented with education and lifestyle changes. Get informed about the risks of heart disease and stroke.”
American Heart Association
QUOTE FOR THE WEEKEND:
“They said I was a valued customer, now they send me hate mail.”
― Sophie Kinsella, Confessions of a Shopaholic (a British author and The first two novels in her best-selling Shopaholic series, The Secret Dreamworld of a Shopaholic and Shopaholic Abroad were adapted into the film Confessions of a Shopaholic starring Isla Fisher.)
Shopping Addiction

Shopping addiction actually has a technical term that is called Omniomania. This means compulsive shopping and is perhaps the most socially reinforced of the behavioral addictions. Shopping addiction is characterized by the widespread desire to shop and purchase items despite a need for such items or despite a necessary ability to afford such items. Consumerism is one of the biggest measures of social elite in America and this makes shopping addiction an even more widespread problem for many.
Shopaholics, also known as compulsive shoppers or shopping addicts, may actually be suffering from a psychiatric disorder known as compulsive buying disorder.
Compulsive buying disorder (CBD) sufferers have a sense of excitement before a purchase, an inability to resist the urge to shop and a rush or sense of reward while spending, despite any negative consequences of their actions. CBD is considered an impulse-control disorder. Just as with other impulse-control disorders such as drug and alcohol addiction and pathological gambling, for many compulsive shoppers the “high”of the spending spree is followed by a low, where the powerful euphoric feelings are replaced with those of distress, shame and guilt.
Shopping addiction is not a newfound disorder. It has affected millions of people for many years and dates back to as early as the 19th century. Friends and family members go out and shop together, people shop socially, people shop for something to do and people shop to fulfill negative emotions. An addiction to shopping leads to compulsive shopping that can result in many negative feelings. According to the US National Library of Medicine, over 5% of Americans are affected by compulsive buying disorder.
While some of us may enjoy the thrill of an occasional splurge or scoring a good deal, spending more than you bargained for during an annual holiday shopping spree doesn’t automatically make you a shopaholic. But that thrill, what some shopaholics describe as a high, helps drive compulsive shoppers to want more — excessive shopping, uncontrolled spending sprees and impulse buys are the defining characteristics of compulsive buying disorder.
People who suffer from compulsive buying disorder may also have feelings of anxiety or tension while they try to resist the urge to shop. And unlike those who compulsively shop without regret during the manic periods of bipolar disorder, CBD sufferers often feel depressed or distressed for having given in to the urge and guilty over their growing debts after they’ve gone on a spree. But it can be those very feelings of distress, shame and depression that ignite the shopping addict to again seek the “high” that comes along with shopping, despite any negative consequences of their actions.
The average American has about three credit cards and knows how to use them — on average, a cardholder owes almost $16,000 on their plastic [source: Woolsey]. Compulsive shoppers have, on average, the same number of cards as the rest of us but the difference is that they’re more likely to maintain balances between $100 to $500 shy of each card’s maximum limit [source: Koran]. They shop excessively and impulsively, typically making their purchases on credit.
What’s excessive? Treating yourself to that pair of luxurious new boots you’ve had your eye on may feel excessive and unnecessary, especially if you’re on a tight budget, but compulsive shoppers might buy five, 10 or even 20 pairs of those boots without hesitation. Some shopaholics shop for the thrill of the purchase no matter what the item is. Others may have specific shopping preferences — consider the 2,000 to 3,000 pairs of shoes former first lady of the Philippines Imelda Marcos had collected, for example.
Any debt you can’t (or don’t) pay off quickly is too much debt. While the amount of debt you carry is ultimately going to be a personal decision, there’s a quick way to know for sure how your monthly financial obligations stack up against your monthly income. Add up your monthly debt obligations — that’s your rent or mortgage, your credit card, car loan, student loan and any other loan payments (this does not include what you pay for food, clothing, utilities or your discretionary spending). Add up your monthly income — that’s your gross salary plus any other income such as a bonus or alimony. If less than 30 percent of your income is used to pay your debts, you’re in pretty good shape at the moment. When the ratio begins to creep towards 40 percent or greater, though, it’s time for a financial intervention.
Do you think about shopping every day? Do you shop for yourself every day or every week? Do you understand why you shop – what drives it, what triggers it, and what consequences it has (could you write those things down or cogently describe them to someone else)? Do you ever feel bad (guilty, ashamed, fearful) after a shopping trip? Do you ever feel weirdly ‘up’ after a shopping trip (triumphant, exultant, complete)? Does shopping fill a lot of your time, thoughts and creative energy? Does shopping take a large portion of your disposable income? Is your relationship to shopping one of your most important? Do you have significant credit card debt, racked up on clothing, shoes and accessories purchases? Are you on a first name basis with the sales people of your favourite stores, you shop there so much? Do you have the phone numbers of your favourite stores on speed dial? Is the thought of not going shopping for any period of time (a month, 6 months, a year) cause you to feel light-headed, heavy-hearted or short-of-breath with the sheer mortification of it? Who’s the boss – shopping or you?
If you say yes to a lot of these questions or just know shopping is the boss than you have a shopping problem and it’s up to you only to make the choice in making this shopaholic habits be put to rest and allow you to control your own life not shopping control you. Good luck if you have or now know you have a problem.
How do you resolve it control it yourself or go to a doctor or psychologist or psychiatrist or even a specialist who majors in counseling people with this problem.
QUOTE FOR FRIDAY:
“Most cases of colon cancer begin as small, noncancerous (benign) clumps of cells called adenomatous polyps. Over time some of these polyps become colon cancers.”
MAYO CLINIC
QUOTE FOR THURSDAY:
“Many STDs cause no symptoms in some people, which is one of the reasons experts prefer the term “sexually transmitted infections” to “sexually transmitted diseases.”
MAYO CLINIC