


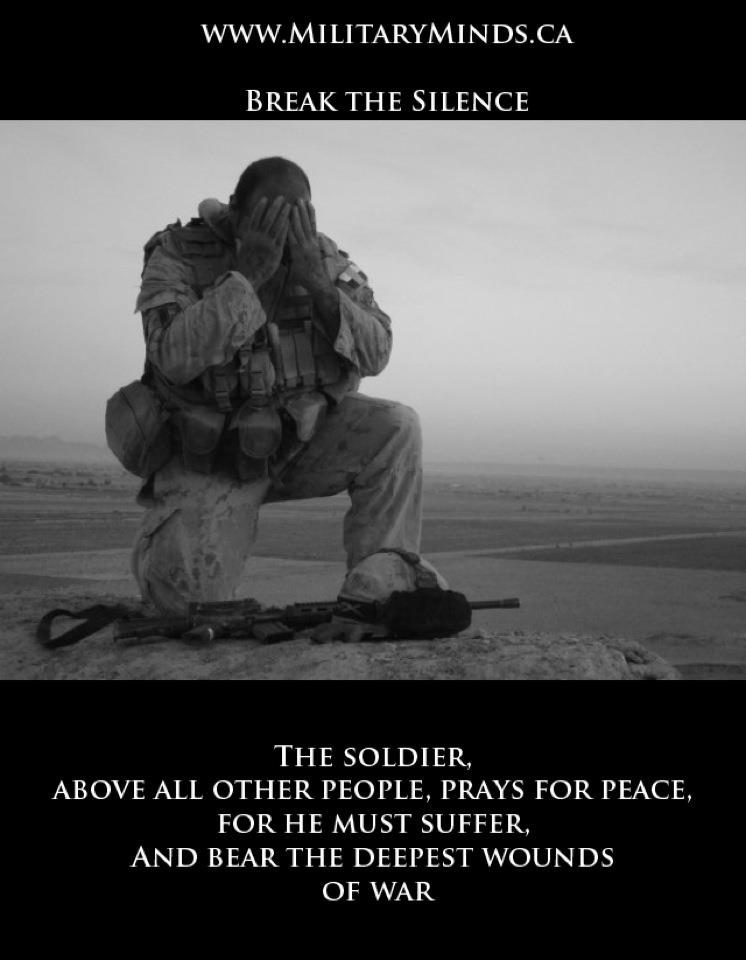
Many risk factors revolve around the nature of the traumatic event itself!
Traumatic events are more likely to cause PTSD when they involve a severe threat to your life or personal safety: the more extreme and prolonged the threat, the greater the risk of developing PTSD in response. Intentional, human-inflicted harm—such as rape, assault, and torture— also tends to be more traumatic than “acts of God” or more impersonal accidents and disasters. The extent to which the traumatic event was unexpected, uncontrollable, and inescapable also plays a role.
PTSD can happen to anyone. It is not a sign of weakness. A number of factors can increase the chance that someone will have PTSD, many of which are not under that person’s control. For example, having a very intense or long-lasting traumatic event or getting injured during the event can make it more likely that a person will develop PTSD. PTSD is also more common after certain types of trauma, like combat and sexual assault.
Personal factors, like previous traumatic exposure, age, and gender, can affect whether or not a person will develop PTSD. What happens after the traumatic event is also important. Stress can make PTSD more likely, while social support can make it less likely.
What factors affect Veterans who develops PTSD?
– PTSD can happen to anyone. It is not a sign of weakness. A number of factors can increase the chance that someone will have PTSD, many of which are not under that person’s control. For example, having a very intense or long-lasting traumatic event or getting injured during the event can make it more likely that a person will develop PTSD.
PTSD is also more common after certain types of trauma, like combat and sexual assault.
– Personal factors, like previous traumatic exposure, age, and gender, can affect whether or not a person will develop PTSD. What happens after the traumatic event is also important. Stress can make PTSD more likely, while social support can make it less likely.
– Women changing roles in our military
A growing number of women are serving in the US military. In 2008, 11 of every 100 Veterans (or 11%) from the Afghanistan and Iraq military operations were women. These numbers are expected to keep rising. In fact, women are the fastest growing group of Veterans.
– Know this, MALES experience more traumatic events on average than do females, yet females are more likely to meet diagnostic criteria for Post Traumatic Stress Disorder (PTSD), according to a review of 25 years of research reported in the November issue of Psychological Bulletin, published by the American Psychological .
– The lifetime prevalence of PTSD is 10% to 12% in women and 6% to 8% in men. Traumatic events happen to both sexes and can result in the same symptoms. The differences depend on when the trauma happens, what type of trauma it is, and biological factors unique to women versus men. These things determine whether someone who goes through trauma develops PTSD.
– High-impact trauma is a severe type of trauma likely to lead to PTSD symptoms.
Women are generally exposed to more high-impact trauma than men are based on reports. One of the traumas most likely to lead to PTSD is sexual assault. Know one in four women are raped by age 44; 8% of men are.
Women are also more likely to experience sexual abuse at an earlier stage of life. The earlier a person experiences trauma, the more it impacts personality and brain development.
Women are also more likely to experience other high-impact traumas, like domestic violence.
One of the reasons these types of trauma are more likely to lead to PTSD is because feelings of shame and self-blame often accompany sexual and interpersonal violence. While men also experience traumas like sexual assault, abuse, and domestic violence, they do so at a lower rate.
– Combat trauma, which PTSD is most associated with, affects men much more often than it does women. It also generally produces less shame and other negative feelings about oneself. The same is true for car accidents and natural disasters.
What stressors do women face in the military?
Here are some stressful things that women have experienced when in the military or might have gone through while deployed:
-Combat Missions even though more men have experienced combat PSTD in research some women have as well.
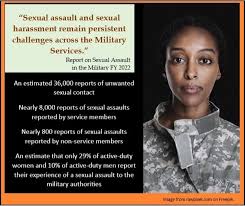
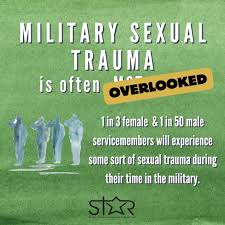
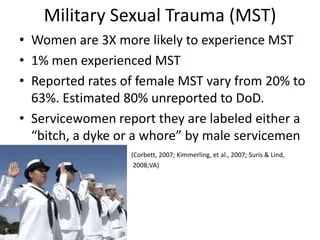
-Military Sexual Trauma (MST). A number of women and men who have served in the military experience MST. MST includes any sexual activity where you are involved against your will, such as insulting sexual comments, unwanted sexual advances, or even sexual assault.
-Feeling Alone. In tough military missions, feeling that you are part of a group is important.
-Worrying About Family. It can be very hard for women with young children or elderly parents to be deployed for long periods of time. Service members are often given little notice. They may have to be away from home for a year or longer. Some women feel like they are “putting their lives on hold.”
Because of these stressors, many women who return from deployment have trouble moving back into civilian life. While in time most will adjust, a small number will go on to have more serious problems like PTSD.
How many women Veterans have PTSD?
Among women Veterans of the conflicts in Iraq and Afghanistan, almost 20 of every 100 (or 20%) have been diagnosed with PTSD. We also know the rates of PTSD in women Vietnam Veterans. An important study found that about 27 of every 100 female Vietnam Veterans (or 27%) suffered from PTSD sometime during their postwar lives.
To compare, in men who served in Vietnam, about 31 of every 100 (or 31%) developed PTSD in their lifetime.
Signs and Symptoms of PTSD for anyone experiencing this disorder:
PTSD symptoms usually start soon after the traumatic event, but they may not appear until months or years later. They also may come and go over many years. If the symptoms last longer than four weeks, cause you great distress, or interfere with your work or home life, you might have PTSD.
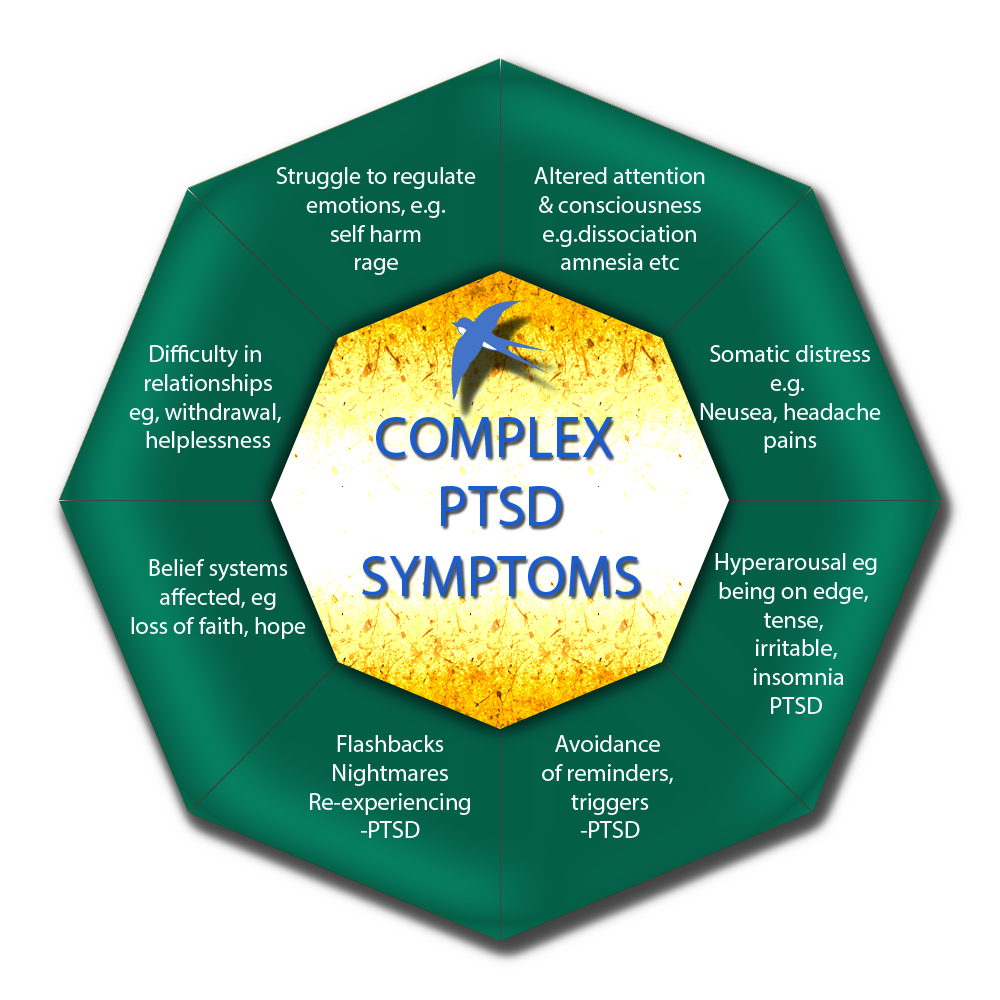
There are four types of symptoms of PTSD, but they may not be exactly the same for everyone. Each person experiences symptoms in their own way.
- Reliving the event (also called re-experiencing symptoms). You may have bad memories or nightmares. You even may feel like you’re going through the event again. This is called a flashback.
- Avoiding situations that remind you of the event. You may try to avoid situations or people that trigger memories of the traumatic event. You may even avoid talking or thinking about the event.
- Having more negative beliefs and feelings. The way you think about yourself and others may change because of the trauma. You may feel guilt or shame. Or, you may not be interested in activities you used to enjoy. You may feel that the world is dangerous and you can’t trust anyone. You might be numb, or find it hard to feel happy.
- Feeling keyed up (also called hyperarousal). You may be jittery, or always alert and on the lookout for danger. Or, you may have trouble concentrating or sleeping. You might suddenly get angry or irritable, startle easily, or act in unhealthy ways (like smoking, using drugs and alcohol, or driving recklessly.



{kind=link}