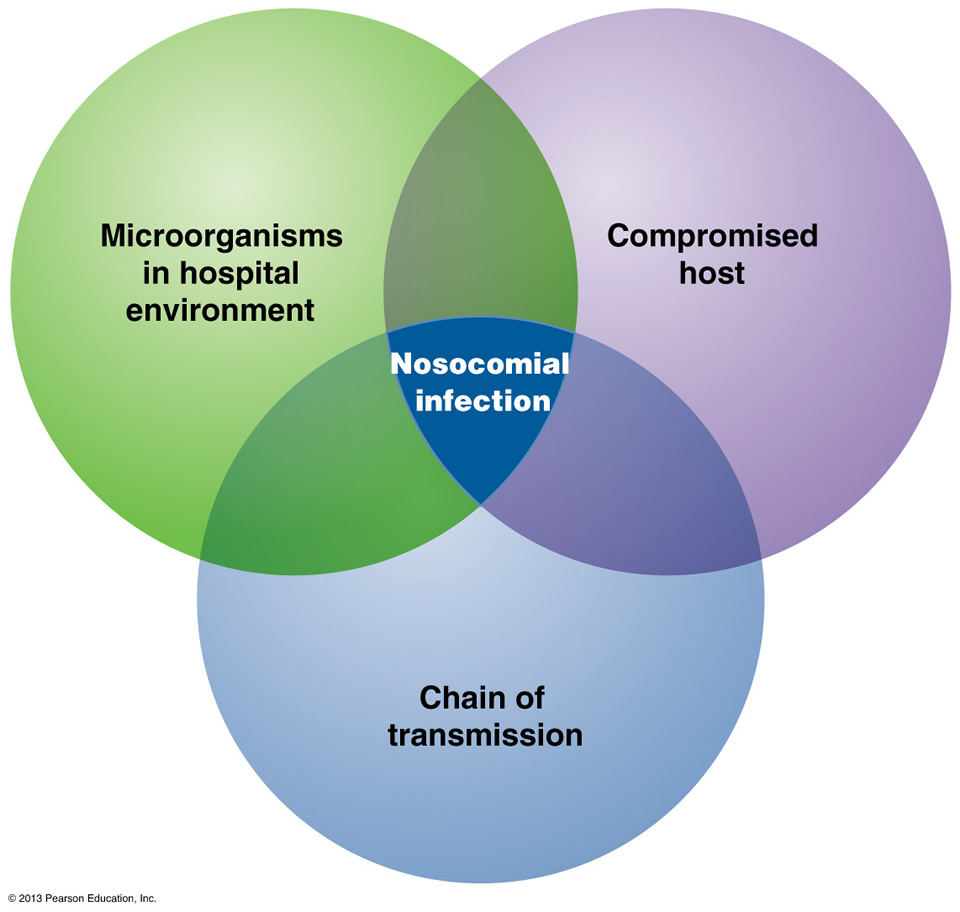
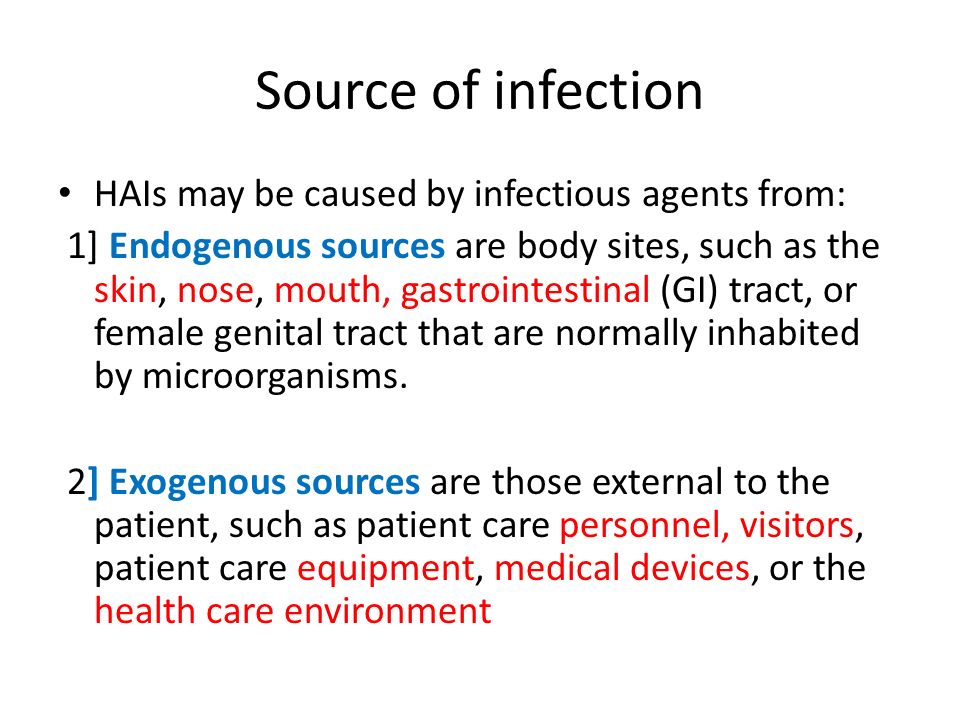

Factors and types of procedures that put an individual at risk for HAIs:
*Healthcare facilities, including hospitals, acute care facilities, and long-term care facilities, contain many organisms and methods of transfer of bacteria; however, certain infections occur more frequently than others in healthcare environment.
*The most common pathogens causing catheter associated urinary tract infections (CAUTIs) are E. coli, Candida spp., Enterococcus spp., Pseudomonas aeruginosa, Klebsiella pneumoniae, and Enterobacter spp. Pathogens may gain access to the urinary system during insertion, manipulation, maintenance, or removal of a urinary catheter. Pathogens enter the urinary tract via the extra-luminal route, by moving along the outside of the catheter getting up in the urethra back up in the urinary bladder and something not sterile or even clean got up into a area that is causing risk of infection.
Studies show that by the 30th day of catheterization, which is also considered the demarcation between short- and long-term catheterization the daily risk, of bacteria in the urine approaches to 100%. In a acute hospital if a patient has a catheter applied for surgery it is out the next day or two and if not many facilities have MDs having to renew the order in the patient’s chart or its removed if the intial order stated the time it starts and the time the orders ends (usually in 48 hrs), again if it is a simple operation (ex. A pacemaker insertion with no post-op difficulties as opposed to a patient who has CABG-coronary artery bypass graft surgeRemember in most cases there’s several factors putting many people at higher risk for the UTIs, here are some examples:
*Certain women – One major reason for this is because the urethra in all women is shorter than in men, this cuts down on the distance for urine in the urinary bladder to reach the end of the urethra where the urine comes out. This allows bacteria to take a shorter route to enter a women in reaching her bladder going back up the urethra and putting her at higher risk of infection. Also women more sexually active is at higher risk for UTIs also cause of the same reason again due to a shorter urethra.
`*AGE -the older adults and those with prolonged catheterization (infection begins when an organism successfully colonizes by entering the body, growing and multiplying). Medical conditions that increase the risk of a CAUTIs include diabetes, diarrhea, renal insufficiency, and a compromised immune system. Colonization of the catheter drainage bag can also increase a patient’s risk for a CAUTIs (the reason to get it out of the patient as soon as possible, if the patient is a candidate for removal). A patient for example that may not be a candidate and leaving it in for 2 weeks or more is a patient who is incontinent but let’s say is in the hospital with a open wound to the lower back or buttock or hip but if urine gets into the wound it will just infect it so to prevent urine incontinency from touching the wound the foley catheter is inserted as a diversion. When the wound heals it’s immediately discontinued and taken out of the patient, for example.
If a bacteria infection is presented (a UTI) than the patient should be started on a antibiotic that only kills bacterial infections. The patient should stay on the medication 7 to 14 days.
* Central Line-Associated Bloodstream Infections-Perhaps the most deadly HAI, central line–associated bloodstream infections (CLABSIs) are transmitted via a central venous catheter (CVC) directly to a patient’s bloodstream. A CVC is any intravascular catheter that terminates at or close to the heart or in one of the great vessels and is used for infusion of medications, nutrition, and blood; withdrawal of blood; hemodialysis access; and hemodynamic monitoring. CVCs may be placed in the large veins of the chest (through axillary or subclavian veins), the neck (through the internal jugular vein), or the groin (through the femoral vein). The infection cannot be related to any other infection the patient might have and must not have been present or incubating when the patient was admitted to the healthcare facility. Tens of thousands of CLABSIs occur in U.S. hospitals each year, with deadly results: Up to 25% of those diagnosed with a CLABSI will die from the infection. Unfortunately a significant number of these infections continue to occur in inpatient settings and in hemodialysis facilities, even though most CLABSIs, especially those occurring in ICUs, are preventable. The longer the patient has a central line, the more likely he or she is to acquire a bloodstream infection via the line. The type of material the catheter is made from also affects infection transmission. Infection risk is also increased in patients with concurrent infection and those treated in the ICU.
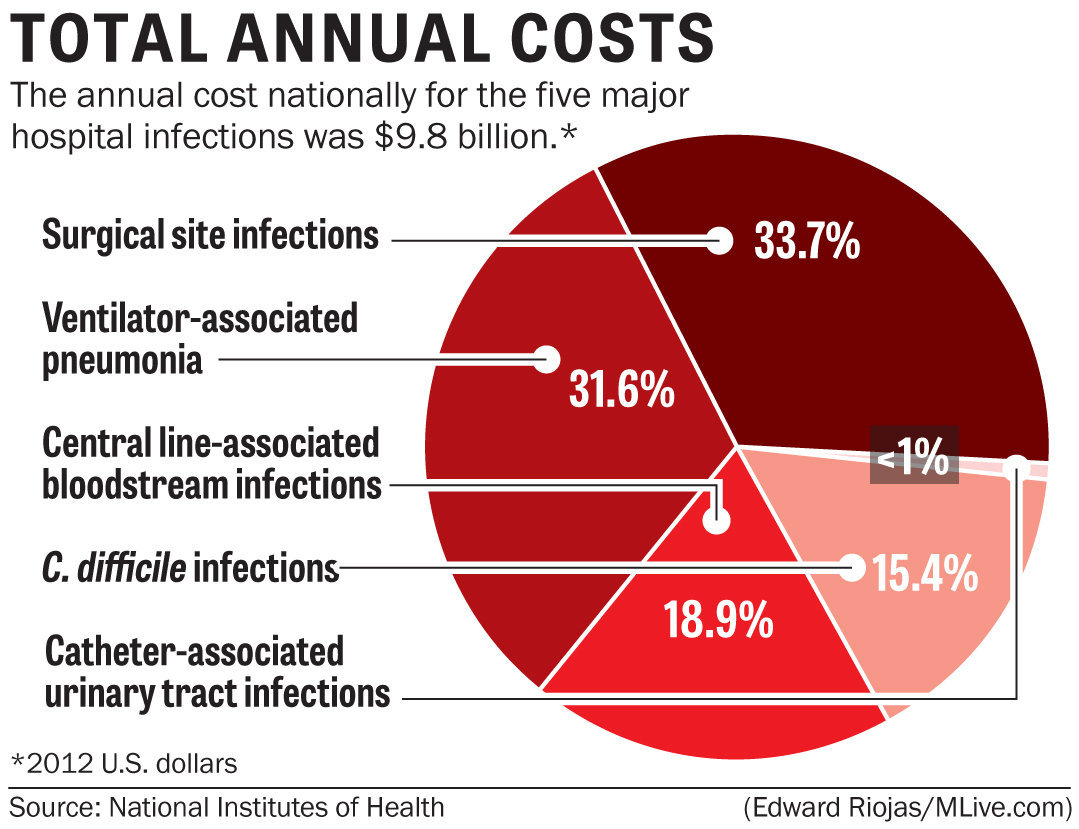
*Surgical Skin Infections (SSIs) – Anytime the skin barrier is broken, the risk for infection rises, so it is only logical that surgery will increase a patient’s risk for a HAI. Surgical site infections (SSIs) occur at the location where a surgery was previously performed. To be diagnosed as a SSI, the infection must occur within 30 days of surgery if no implant is left in place or within 1 year if the implant is in place and the infection appears to be related to the operative procedure.
*Ventilator-associated pneumonia (VAP) is an infection of the lungs that develops after a person has been on a ventilator for longer than 48 hours. The most common type of HAI contracted in the ICU, VAP occurs in as many as 28% of patients who have had mechanical ventilation. Infection occurs because the endotracheal or tracheostomy tube allows passage of microbes into the lungs. These organisms may originate from the patient’s aspirate, from the oropharynx and digestive tract, or from external sources, such as contaminated equipment and medications.
Although any microbe can be the causative agent, certain microbes are most often implicated due to increasing drug resistance. Pseudomonas aeruginosa is the most common multidrug-resistant organism responsible for VAP. Other microbes that cause VAP include Staphlococcus aureus, Klebsiella spp., Escherichia coli, Enterobacter spp., Actinobacter spp., MRSA, and Serratia marcescens. Pneumonia is considered early in onset if it occurs within the first 4 days after hospital admission. Multidrug resistant organisms are more likely to be the cause of late-onset pneumonia, defined as 5 or more days post-admission.
In addition to recent ventilation, other risk factors increase a patient’s chance of acquiring VAP, such as hospitalization or antibiotic use within the past 90 days, hospital stay greater than 5 days, hemodialysis within the past 30 days, and known circulation of multidrug-resistant organisms in the facility. Immuno-compromised residents and those who reside in a nursing home or long-term care facility are also at greater risk for VAP. Empiric treatment is vital in patients with suspected VAP and can be based on patient risk factors for multidrug-resistant organisms, known local prevalence of resistant organisms, severity of infection, and total number of days the patient was hospitalized before the onset of pneumonia. Unless diagnostic testing shows otherwise, initial empiric therapy should not be changed in the first 48 to 72 hours because clinical response to antibiotic therapy is not likely during this time frame. Patients should be treated with antibiotic therapy for at least 72 hours after a clinical response is attained. To prevent VAP, the CDC recommends the following strategies:
Strategies to Prevent Aspiration
- Maintain patients in a semirecumbent position.
- Avoid gastric overdistention.
- Avoid unplanned extubation and reintubation.
- Use a cuffed endotracheal tube with inline or subglottic suctioning.
- Maintain an endotracheal cuff pressure of at least 20 cm water.
Strategies to Reduce Colonization of the Aerodigestive Tract
- When possible, use orotracheal intubation rather than nasotracheal intubation.
- Avoid histamine receptor 2 (H2)–blocking agents and proton pump inhibitors for patients who are not at high risk for developing a stress ulcer or stress gastritis.
- Perform regular oral care with an antiseptic solution.
Strategies to Minimize Contamination of Equipment
- Use sterile water to rinse reusable respiratory equipment.
- Remove condensate from ventilatory circuits, keeping the ventilatory circuit closed while you do so.
- Change the ventilatory circuit only when visibly soiled or malfunctioning.
- Store and disinfect respiratory therapy equipment properly.
In addition to these strategies, healthcare professionals should perform daily assessments of readiness to wean to minimize the duration of ventilation. Whenever possible, use noninvasive ventilation methods.
See tomorrow’s Part 3 on HAIs discussing actual names of infections that we deal with in health facilities and learn about them to be prepared if, unfortunately, you, your family or friends have to go to one.