“Anemia is a condition in which you don’t have enough healthy red blood cells to carry adequate oxygen to the body’s tissues. Having anemia may make you feel tired and weak”
MAYO CLINIC
“Anemia is a condition in which you don’t have enough healthy red blood cells to carry adequate oxygen to the body’s tissues. Having anemia may make you feel tired and weak”
MAYO CLINIC
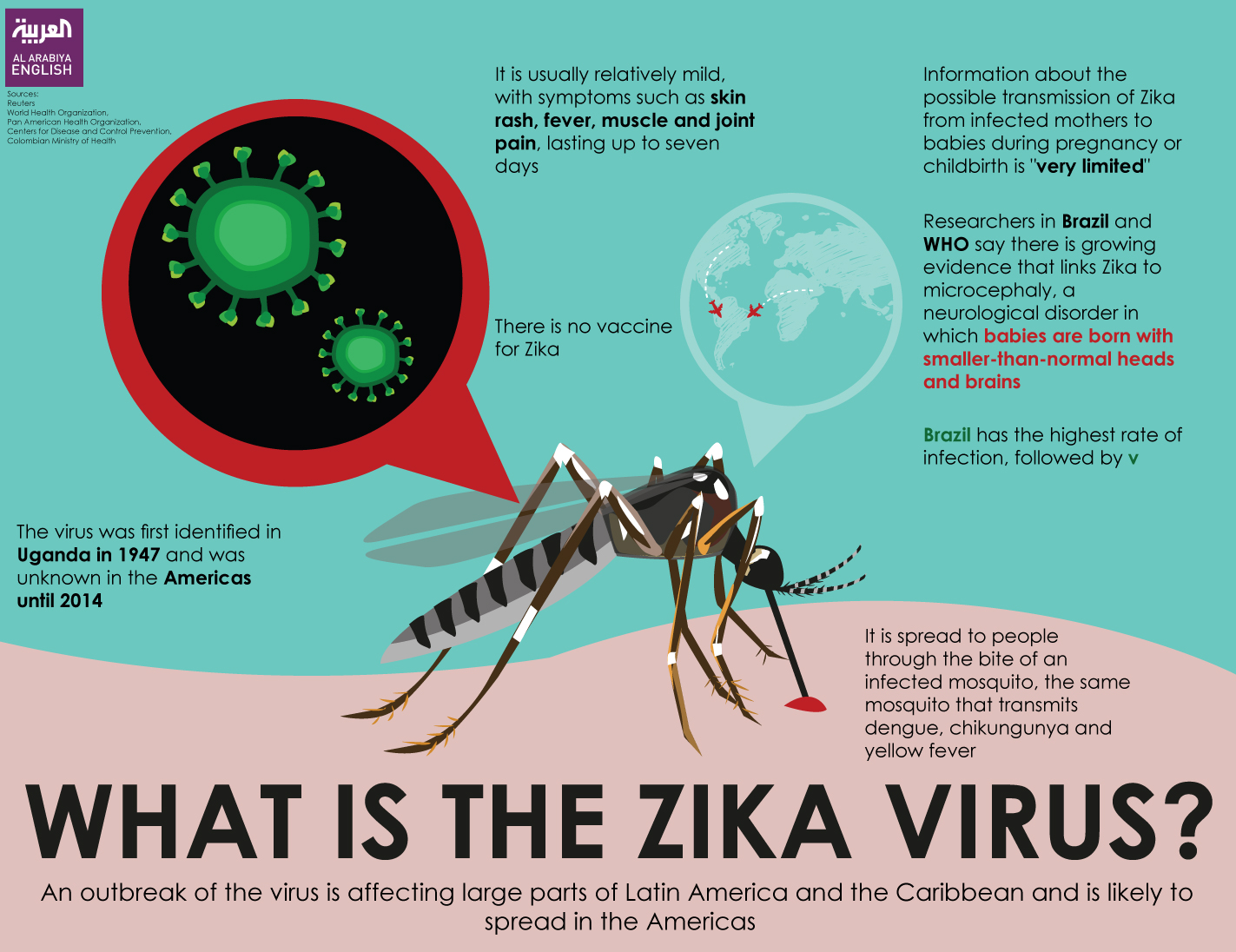
“Several years ago, it was all about West Nile and now Zika virus. All kinds of celebrities are engaged in solutions to Malaria for third world countries. Obviously, we’re familiar with all of them. But which disease are you most likely to get and which are you most likely to recuperate from?
A little bit of background on mosquitoes. They must have water to lay eggs. It doesn’t need to be much water at all – just enough to fill the palm of your hand. The mosquitoes lay eggs that hatch into water-loving larva. The larval stage is brief – only 3 days or so – and water is the essential ingredient.”
Greenbugallnatural
West Nile Virus 
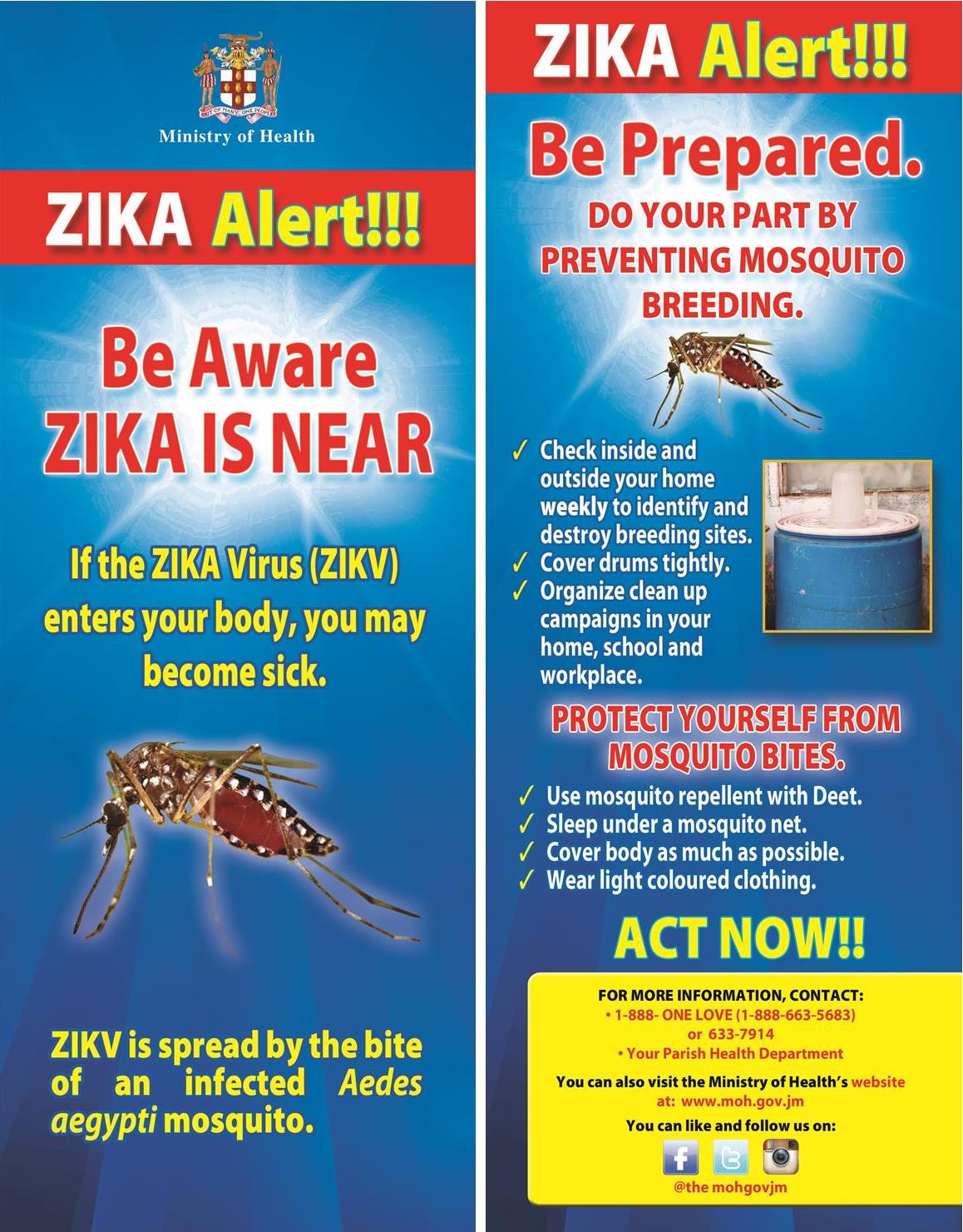
The Department of Health in New York is taking action against mosquitoes who spread the Zika virus with the West Nile Virus. Zika Virus is an epidemic already in Florida but NYC is trying to stop this. How? Well AM radio station 1010Wins stated yesterday that Tonight at 10pm till the am and now Fox news states tomottow at 6am the action will start; which is pesticides in the air will be dropped in the sky for hours to prevent amid growing concern of these mosquitoes spreading Zika or West Nile Virus to New York City areas. Hopefully other areas of NY and the NE will be prevented long before a cases show up before the other cities/towns take action.
While assuring residents that the virus is not spreading in New York City, it says local mosquitoes are spreading other diseases like the West Nile Virus.
With mosquito season upon us, the city is going to begin a three day aerial bombardment of marsh and other non-residential areas at some two dozen sites in the Bronx, Queens, Staten Island and Brooklyn Fox News states but all 5 buroughs covered 1010 wins states also.
Officials say they will use “environmentally friendly” larvicide to kill the infant mosquito larvae.
With projected hot and damp weather the mosquito population is expected to have huge growth this season.
Residents Fox News spoke to in Marine Park, Brooklyn said they were concerned and relieved that the city is taking action.
Mike Nagar said he’s skeptical about how safe the chemicals are that will be sprayed but would you rather be diseased with Zika or West Nile Virus or God knows what if no action is taken place.
Standing beside his pregnant wife, Daniel Cicolello said he’s concerned because the mosquito-borne Zika virus impacts pregnant women.
Those so terribly concerned should ease their conscious and get out of NY for TH,FRI and the Weekend and come home on SUN or deal with infection control measures rather than do nothing.
It is known to cause birth defects. It is not considered dangerous for most people and action to prevent an epidemic is a must to prevent a negative domino effect spreading it on or too many people or everyone to kill some and get others terribly sick with continuous spreading. If the mosquitoes don’t get controlled neither will the Zika or West Nile Virus.
Health officials note that there have been 78 cases of Zika reported in the city, but that all the patients have recovered.
“I now realize that I have a platform to inspire young girls, and as someone who never had a role model who looked like me when I was growing up, I now hope to be able to show that albinism can be beautiful and is just another kind of normal.”
Thando Hopa (#SouthAfrican #African #Africa #Motherland #Model #Albino)



The word “albinism” refers to a group of inherited conditions. People with albinism have little or no pigment in their eyes, skin, or hair. They have inherited altered genes that do not make the usual amounts of a pigment called melanin. One person in 17,000 in the U.S.A. has some type of albinism. Albinism affects people from all races. Most children with albinism are born to parents who have normal hair and eye color for their ethnic backgrounds. Sometimes people do not recognize that they have albinism. A common myth is that people with albinism have red eyes. In fact there are different types of albinism and the amount of pigment in the eyes varies. Although some individuals with albinism have reddish or violet eyes, most have blue eyes. Some have hazel or brown eyes. However, all forms of albinism are associated with vision problems.
Vision Problems
People with albinism always have problems with vision (not correctable with eyeglasses) and many have low vision. The degree of vision impairment varies with the different types of albinism and many people with albinism are “legally blind,” but most use their vision for many tasks including reading and do not use Braille. Some people with albinism have sufficient vision to drive a car. Vision problems in albinism result from abnormal development of the retina and abnormal patterns of nerve connections between the eye and the brain. It is the presence of these eye problems that defines the diagnosis of albinism. Therefore the main test for albinism is simply an eye examination.
Skin Problems
While most people with albinism are fair in complexion, skin or hair color is not diagnostic of albinism. People with many types of albinism need to take precautions to avoid damage to the skin caused by the sun such as wearing sunscreen lotions, hats and sun-protective clothing.
Types of Albinism
While most people with albinism have very light skin and hair, not all do. Oculocutaneous (pronounced ock-you-low-kew-TAIN-ee-us) albinism (OCA) involves the eyes, hair and skin. Ocular albinism (OA), which is much less common, involves primarily the eyes, while skin and hair may appear similar or slightly lighter than that of other family members.
Over the years, researchers have used various systems for classifying oculocutaneous albinism. In general, these systems contrasted types of albinism having almost no pigmentation with types having slight pigmentation. In less pigmented types of albinism, hair and skin are cream-colored and vision is often in the range of 20/200. In types with slight pigmentation, hair appears more yellow or red-tinged and vision may be better. Early descriptions of albinism called these main categories of albinism “complete” and “incomplete” albinism. Later researchers used a test that involved plucking a hair root and seeing if it would make pigment in a test tube. This test separated “ty-neg” (no pigment) from “ty-pos” (some pigment). Further research showed that this test was inconsistent and added little information to the clinical exam.
Recent research has used analysis of DNA, the chemical that encodes genetic information, to arrive at a more precise classification system for albinism. Four forms of OCA are now recognized – OCA1, OCA2, OCA3 and OCA4; some are further divided into subtypes.
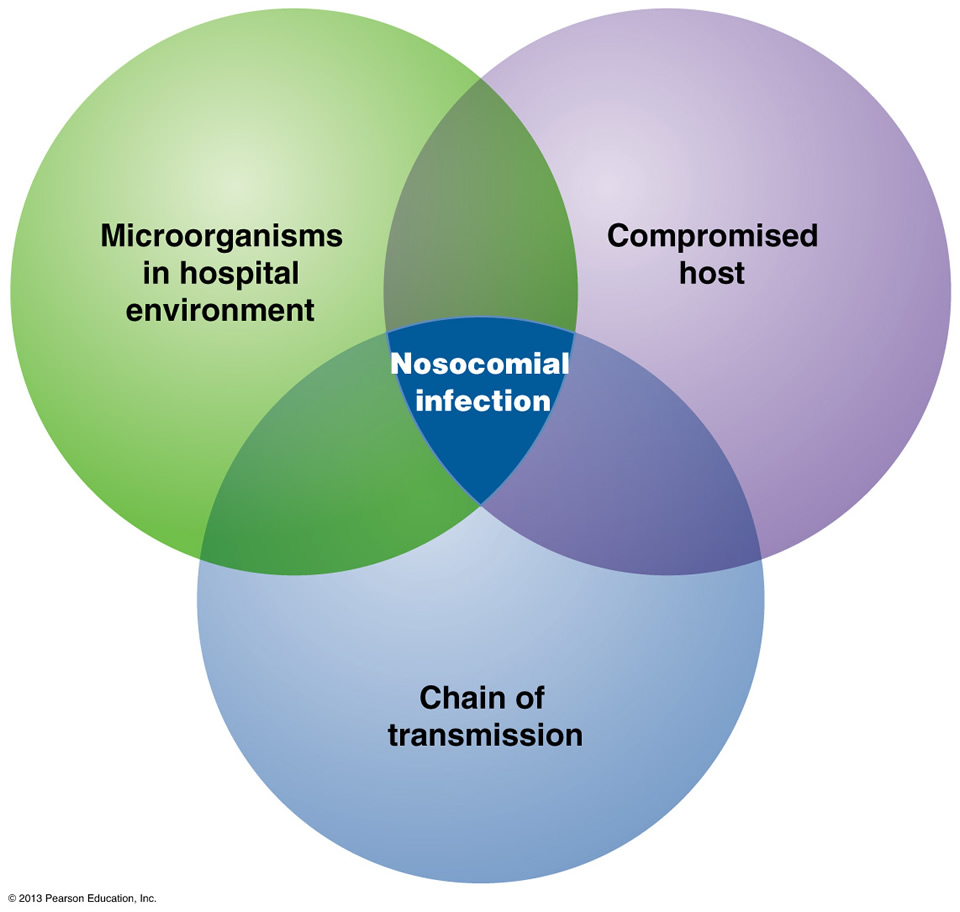
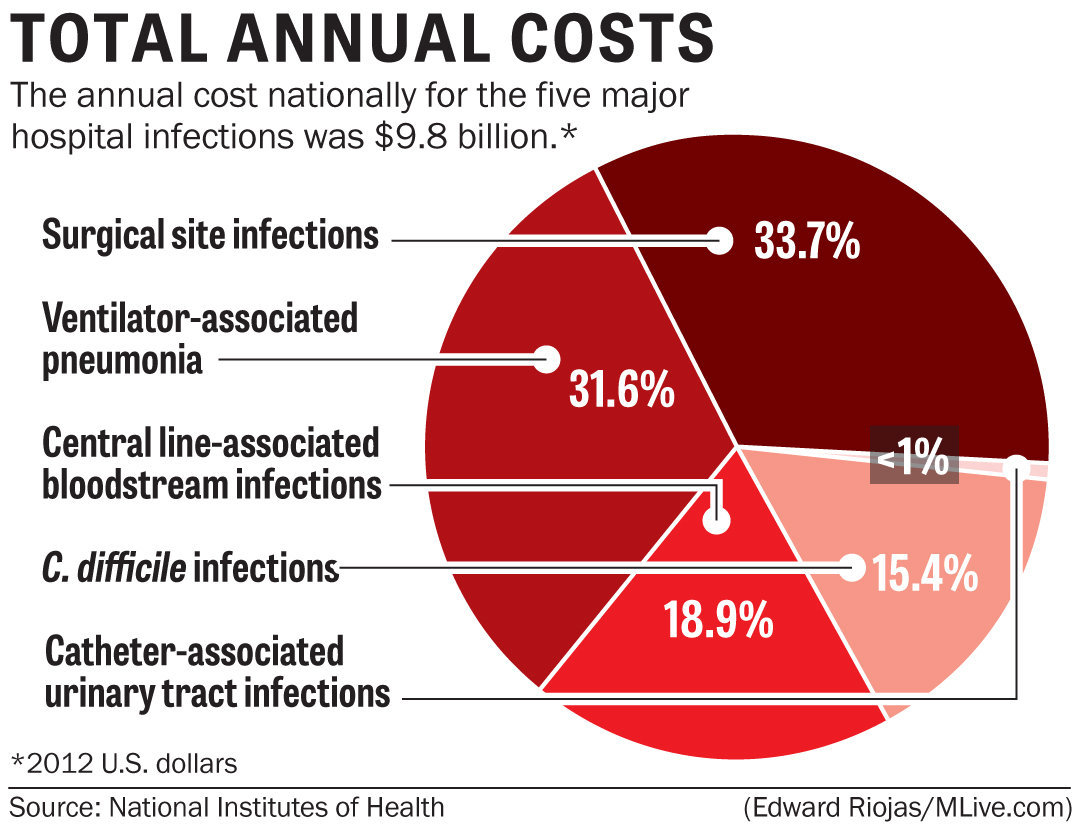
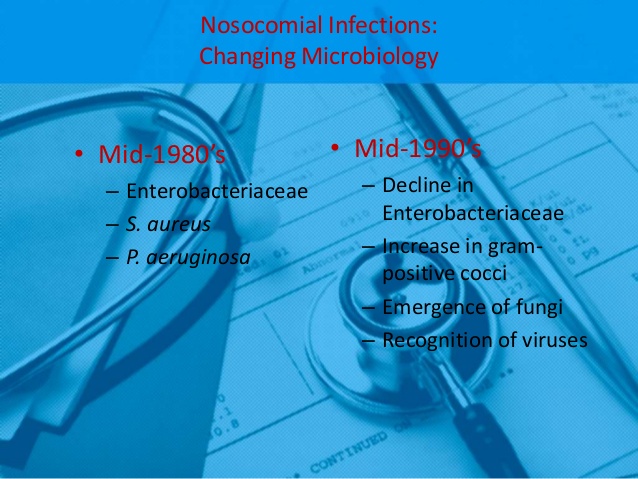
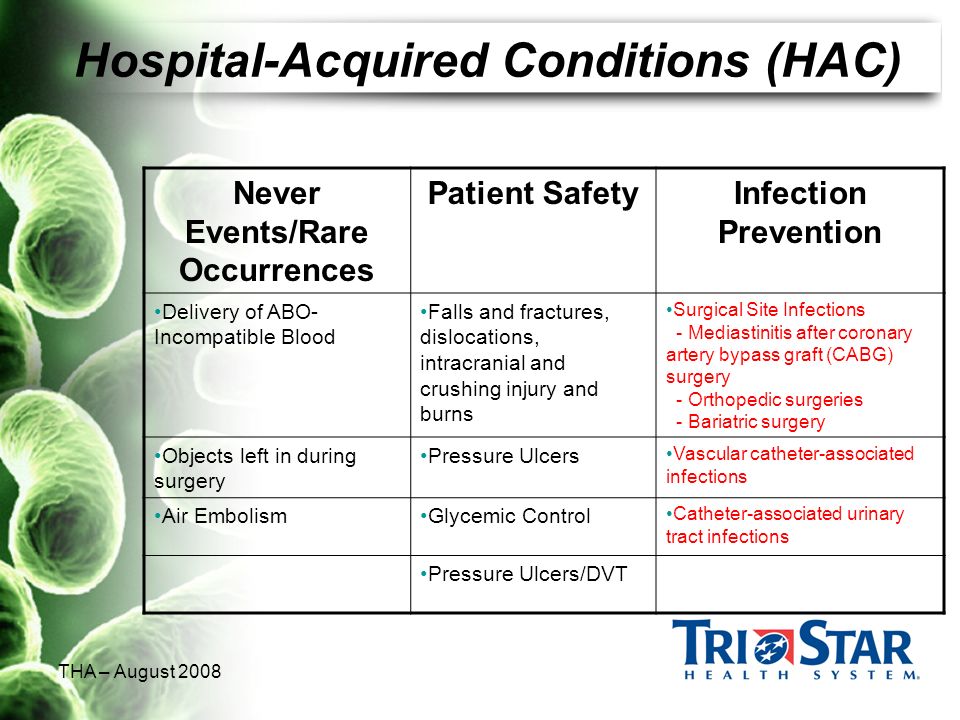
“Health care-associated infections, or HAIs, are infections that people acquire while they are receiving treatment for another condition in a health care setting. HAIs may be caused by any infectious agent, including bacteria, fungi, and viruses, as well as other less common types of pathogens.”
Office of disease prevention and health promotion
THE KEY is to not allowing a Health Acquired Infection-HAI to even occur; this is through PREVENTION!
To reach this key is to understand exactly what a HAI is and how they work in spreading. If you didn’t get a chance to read Tues. Part 1, Wed. Part 2 and Thurs. Part 3 articles do that first to learn what HAIs actually are. The public has to get focused.
Prevention with the most common HAI is UTIs, the CDC recommends healthcare workers to do the following:
“More action is needed at every level of public health and health care to improve patient safety and eliminate infections that commonly threaten hospital patients.”
CDC (Center for disease control and prevention).
1-C-DIFF or C-difficile, know as Clostridium difficile infection (CDI), or Clostridium difficile–associated disease (CDAD), which is an infection of the intestines caused by the anaerobic, spore-forming, gram-positive bacillus C. difficile. This microbe was first identified in 1935 when it was isolated from the stools of neonates. C. difficile produces heat-resistant spores that can remain viable on fomites in the environment for years, becoming a source of outbreaks in healthcare facilities. This bacillus also produces two types of toxins: Toxin A (an enterotoxin) and Toxin B (a cytotoxin). These toxins are responsible for the inflammatory responses of the colon, which results in loss of epithelial integrity and the production of watery diarrhea. C. difficile is the most common cause of antibiotic-associated diarrhea and pseudomembranous colitis and has proved extremely difficult to control due to new, more resistant strains.
Studies of hospital-acquired CDI have shown that the infection is independently associated with increased risk of in-hospital death: For every 10 hospital patients who acquire a CDI, 1 patient died. Data from the CDC show that C. difficile is responsible for 337,000 infections and 14,000 deaths in the United States each year.
The greatest risk factor for CDI is the use of antibiotics, such as cephlasporins, clindamycin, or the penicillins, because these antibiotics kill the normal flora of the colon, causing overgrowth of C. difficile. Risk is increased for those taking multiple antimicrobials and those who take antimicrobials for longer time periods. Other risk factors for CDI include advanced age. Although almost half of the infections occur in persons younger than 65, most CDI-related deaths occur in the elderly. People with HIV infection, compromised immune systems, and compromised physical status are also at increased risk for CDI. Hospital admission increases one’s chance of acquiring CDI, as does gastrointestinal surgery.
Transmission of CDI occurs by the fecal-oral route.
The time between exposure to C. difficile and infection is 2 to 3 days. Symptoms of CDI vary greatly, ranging from asymptomatic to mild (fever, malaise, and gastrointestinal symptoms, including abdominal pain and cramps, and mild to moderate foul-smelling diarrhea that is rarely bloody) to extremely severe toxic megacolon, septic shock, and even death. Complications of C. difficile include pseudomembranous colitis or fulminant colitis.
Diagnosis is based on clinical history (antibiotic use in the previous 2 months, diarrhea after 72 or more hours of hospitalization), and presence of C. difficile in the stool. Stool culture is the most sensitive test and is often used for diagnosis in the hospital setting. Colonoscopy revealing histopathology with pseudomembranous colitis is also diagnostic but not necessary in most cases.
Treatment for CDI begins with discontinuation of the antibiotic causing the infection. In many cases, this step is the only necessary treatment since normal flora can reestablish in the colon. If mild to moderate diarrhea persists, patients can be treated with either metronidazole or vancomycin. In cases of severe diarrhea, vancomycin is the drug of choice for treatment due to its history of rapid symptom resolution and overall fewer treatment failures. Although antibiotic treatment will clear the infection, it will not kill the bacterial spores. In 27% of cases, relapse occurs within 3 weeks of antibiotic termination. In extreme cases, colectomy with end ileostomy may be necessary. Treatment for asymptomatic cases is not recommended.
An innovative CDI treatment may be on the horizon. Researchers have shown that C. difficile infection arises as the result of the disruption of natural flora in the intestines, a condition known as dysbiosis. New research in the treatment of CDI involves isolating specific gut bacteria in the fecal matter of healthy individuals and incorporating it into the gut of a person with CDI to restore normal flora and cure the infection.
CDI can be catastrophic to patients and indeed to entire healthcare facilities if an outbreak occurs. To prevent CDI, follow these guidelines from the CDC:
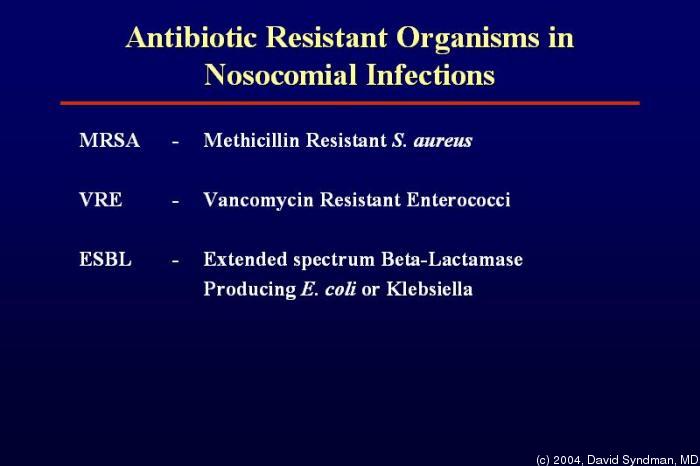
2- MRSA Methicillin-resistant Staphylococcus aureus (MRSA), also known as multidrug resistant S. aureus, includes any strain of S. aureus that has become resistant to the group of antibiotics known as beta-lactam antibiotics. Included in this group are the penicillins (methicillin, amoxicillin, oxacillin) and cephalosporins. Staphylococcus aureus includes gram-positive, nonmotile, non-spore-forming cocci that can be found alone, in pairs, or in grapelike clusters.
When penicillin was first introduced in the early 1940s, it was considered to be a wonder drug because it reduced the death rate from Staphylococcus infection from 70% to 25%. Unfortunately, by 1944, drug resistance was beginning to occur, so methicillin was synthesized, and, in 1959, it became the world’s first semisynthetic penicillin. Shortly thereafter in 1961, staphylococcal resistance to methicillin began as well, and the name “methicillin-resistant S. aureus” and the acronym MRSA were coined. Although methicillin was discontinued in 1993, the name and acronym have remained because of MRSA history.
MRSA is now the most common drug-resistant infection acquired in healthcare facilities. In addition to becoming more problematic as a top HAI in recent years, transmission of MRSA has also become more common in children, prison inmates, and sports participants. Community-associated MRSA (CA-MRSA) most often presents in the form of skin infections. Hospital-acquired MRSA (HA-MRSA) infections manifest in various forms, including bloodstream infections, surgical site infections, and pneumonia. Although approximately 25–30% of persons are colonized in the nasal passages with Staphylococcus, less than 2% are colonized with MRSA. MRSA are extremely resistant and can survive for weeks on environmental surfaces. Transfer of the pathogen can occur directly from patient contact with a contaminated surface or indirectly as healthcare workers touch contaminated surfaces with gloves or hands and then touch a patient.
Risk factors for healthcare-acquired MRSA infection include advanced age, young age, use of quinolone antibiotics, and extended stay in a healthcare facility. Those with diabetes, cancer, or a compromised immune system are also at increased risk of infection.
Symptoms of MRSA infection vary depending on the type and stage of infection and the susceptibility of the organism. Skin infections may appear as painful, red, swollen pustules or boils; as cellulitis; or as a spider bite or bump. They can be found in areas where visible skin trauma has occurred or in areas covered by hair. Patients may also have fever, headaches, hypotension, and joint pain. Complications of MRSA-related skin infections include endocarditis, necrotizing fasciitis, osteomyelitis, and sepsis.
Patient history of admission to a healthcare facility is useful in diagnosing HA-MRSA. Definitive diagnosis of MRSA is made by oxacillin/methicillin resistance that is shown by lab culture and susceptibility testing. Specimens submitted for testing vary depending on the site of suspected infection and may include tissue, wound drainage, sputum, respiratory secretions, and blood or urine cultures.
Treatment for MRSA infections varies based on site of infection, stage of infection, and age of the individual. Treatment includes drainage of abscesses, surgical debridement, decolonization strategies, and antimicrobial therapy with antibiotics such as vancomycin, clindamycin, daptomycin, linezolid, rifampin, trimethoprim-sulfamethoxazole (TMP-SMX), quinupristin-dalfopristin, telavancin, and tetracyclines (limited use). MRSA is rapidly becoming resistant to rifampin; therefore, this drug should not be used alone in the treatment of MRSA infections. Consultation with an infectious disease specialist is recommended for treatment of severe MRSA infections.
3-VRE- Vancomycin-Resistant Enterococci Infection (VRE) or Enterococci (formerly known as Group D streptococci). VRE are non-spore-forming, gram-positive cocci that exist in either pairs or short chains. They are commonly found in the human intestine or the female genital tract. The most common organism associated with vancomycin-ressistant enterococci (VRE) infection in hospitals is Enterococcus faecium. Enterococcus faecalis is also a cause of human disease. VRE infections can occur in the urinary tract, in wounds associated with catheters, in the bloodstream, and in surgical sites. Enterococci are a common cause of endocarditis, intra-abdominal infections, and pelvic infections.
VRE was first reported in Europe in 1986, followed in 1989 by the first report in the United States. Since then it has spread rapidly. Between 1990 and 1997, the prevalence of VRE in hospital patients increased from less than 1% to 15%.
VRE, which is found predominantly in hospitalized or recently hospitalized patients, are difficult to eliminate because they are able to withstand extreme temperatures, can survive for long periods on environmental surfaces, and are resistant to vancomycin. Transmission of VRE occurs most commonly in the form of person-to-person contact by the hands of healthcare workers after contact with the blood, urine, or feces an infected individual. VRE is also spread from contact with environmental surfaces, or through contact with the open wound of an infected person.
People most at risk for infection with VRE include the elderly and those with diabetes, those with compromised immune systems, and those who are already colonized with the bacteria. Prolonged hospitalization, catheterization (urinary and intravenous), and long-term use of vancomycin or other antibiotics also increase a person’s risk of infection.
Symptoms of VRE infection vary depending on the site of infection and may include erythema, warmth, edema, fever, abdominal pain, pelvic pain, and organ pain. Definitive diagnosis is made by culture and susceptibility testing with specimens obtained from suspected sites of infection
“Children and geriatrics are two groups with the highest risk for infection. In addition to age but there are a number of other key risk factors that can contribute to the likelihood of getting a hospital infection. HAIs are one of the biggest public health issues facing society today. Every year, an estimated 1.7 million Americans get a healthcare associated infection, and 99,000 people die as a result of these infections.”
Pennsylvania Dept. of Health