
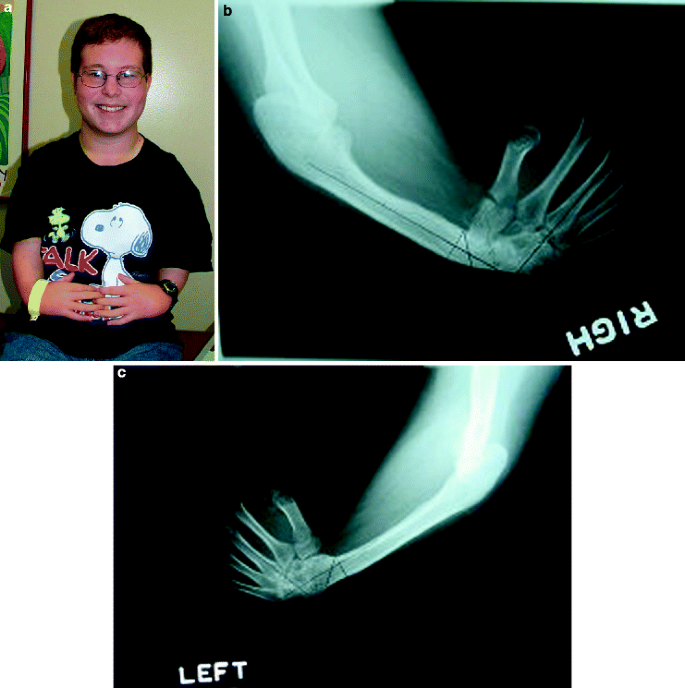
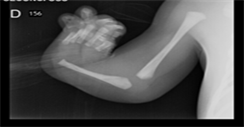


Thrombocytopenia-absent radius (TAR) syndrome is a rare disorder that is present at birth (congenital). It is characterized by low levels of platelets in the blood (thrombocytopenia) and absence (aplasia) of the long, thin bones of the forearms (radii) but with presence of thumbs.
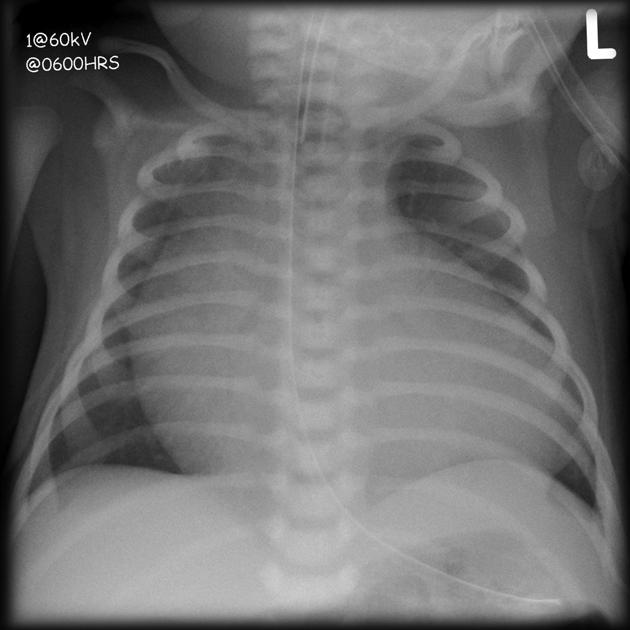
Other abnormalities are often present including additional skeletal defects such as absence or underdevelopment of the other bone of the forearm (ulna), structural malformations of the heart (congenital heart defects) and kidney (renal) defects. Affected individuals may be short for their age (short stature) and have cow’s milk intolerance.
Thrombocytopenia is congenital or develop within the first few weeks to months of life. Usually, platelet counts remain low during the first two years of life; then, they increase but do not normalize. Additional recurrent manifestations include: cardiac anomalies (atrial and/or ventricular septal defect, patent foramen ovale), gastro-intestinal involvement (cow’s milk allergy, increased susceptibility to gastro-enteritis), genitourinary anomalies (kidney agenesis or malrotation, horseshoe kidney, hydronephrosis, pyelectasis). Other rare manifestations include Mayer-Rokitansky-Kuster-Hauser syndrome, rib and vertebral anomalies, Langerhans cell histiocytosis, transient leukemoid reaction, acute myeloid or lymphoblastic leukemia. Cognitive development is usually normal.
The prevalence of thrombocytopenia-absent radius (TAR) syndrome is estimated at around 1/100,000-200,000 people.
Cause of TAR-Thrombocytopenia Absent Radius Syndrome:
TAR syndrome is inherited as an autosomal recessive genetic disorder and caused by deletion and/or variants in the RBM8A gene.
TAR syndrome is caused by compound heterozygosity for a null (most often a 1q21.1 deletion including RBM8A) and a hypomorphic RBM8A allele. It was demonstrated that Rbm8a is an essential neurogenesis regulator in embryonic cortical development. Most people with TAR syndrome have a mutation in one copy of the RBM8A gene and a deletion of genetic material from chromosome 1 that includes the other copy of the RBM8A gene in each cell.
Diagnosing TAR-Thrombocytopenia Absent Radius Syndrome:
It has been reported that TAR syndrome can be accompanied by craniofacial, cardiac, digestive, urogenital, and psychiatric abnormalities, as well as by lactose intolerance(4). The diagnosis of TAR syndrome is based on ultrasound findings and fetal blood sampling by cordocentesis to determine the number of platelets.
Suggestive Findings. Thrombocytopenia absent radius (TAR) syndrome should be suspected in individuals with: Bilateral absence of the radii with the presence of both thumbs. Thrombocytopenia, usually <50 platelets/nL (normal range: 150-400 platelets/nL)
Management and Treatment of TAR-Thrombocytopenia Absent Radius Syndrome:
There is no curative treatment for TAR syndrome. Symptomatic treatment of manifestations and prevention of complications include: early detection of thrombocytopenia, prevention of bleeding and hemorrhage, platelet transfusions in case of severe thrombocytopenia, surgical interventions if required to manage cardiac, urinary or skeletal malformations, avoidance of cow’s milk.
Prognosis of TAR-Thrombocytopenia Absent Radius Syndrome:
Prognosis is variable and mainly conditioned by the severity of thrombocytopenia and its complications (intracranial, digestive hemorrhage). Cardiac defects, renal malformations, acute complications of cow’s milk intolerance, acute leukemia can also affect the prognosis.
If a patient survives the initial 2 years of life, life expectancy is normal, MedLinePlus.com states.
Affected children who survive this period and do not have damaging hemorrhages in the brain usually have a normal life expectancy and normal intellectual development. The severity of skeletal problems in TAR syndrome varies among affected individuals.