Charcot Marie Tooth Disease=CMT is inherited. It is not contagious, nor is it caused by anything in the environment. The most common forms of CMT are passed down from one generation to the next, meaning that it is dominantly inherited.
CMTAUSA.org
Charcot Marie Tooth Disease=CMT is inherited. It is not contagious, nor is it caused by anything in the environment. The most common forms of CMT are passed down from one generation to the next, meaning that it is dominantly inherited.
CMTAUSA.org


Charcot-Marie-Tooth disease (CMT) is one of the most common inherited neurological disorders, affecting approximately 1 in 2,500 people in the United States. The disease is named for the three physicians who first identified it in 1886 – Jean-Martin Charcot and Pierre Marie in Paris, France, and Howard Henry Tooth in Cambridge, England. CMT, also known as hereditary motor and sensory neuropathy (HMSN) or peroneal muscular atrophy, comprises a group of disorders that affect peripheral nerves. The peripheral nerves lie outside the brain and spinal cord and supply the muscles and sensory organs in the limbs. Disorders that affect the peripheral nerves are called peripheral neuropathies.
Causes of Charcot-Marie-Tooth disease?
A nerve cell communicates information to distant targets by sending electrical signals down a long, thin part of the cell called the axon. In order to increase the speed at which these electrical signals travel, the axon is insulated by myelin, which is produced by another type of cell called the Schwann cell. Myelin twists around the axon like a jelly-roll cake and prevents the loss of electrical signals. Without an intact axon and myelin sheath, peripheral nerve cells are unable to activate target muscles or relay sensory information from the limbs back to the brain.
CMT is caused by mutations in genes that produce proteins involved in the structure and function of either the peripheral nerve axon or the myelin sheath. Although different proteins are abnormal in different forms of CMT disease, all of the mutations affect the normal function of the peripheral nerves. Consequently, these nerves slowly degenerate and lose the ability to communicate with their distant targets. The degeneration of motor nerves results in muscle weakness and atrophy in the extremities (arms, legs, hands, or feet), and in some cases the degeneration of sensory nerves results in a reduced ability to feel heat, cold, and pain.
The gene mutations in CMT disease are usually inherited. Each of us normally possesses two copies of every gene, one inherited from each parent. Some forms of CMT are inherited in an autosomal dominant fashion, which means that only one copy of the abnormal gene is needed to cause the disease. Other forms of CMT are inherited in an autosomal recessive fashion, which means that both copies of the abnormal gene must be present to cause the disease. Still other forms of CMT are inherited in an X-linked fashion, which means that the abnormal gene is located on the X chromosome. The X and Y chromosomes determine an individual’s sex. Individuals with two X chromosomes are female and individuals with one X and one Y chromosome are male.
In rare cases the gene mutation causing CMT disease is a new mutation which occurs spontaneously in the individual’s genetic material and has not been passed down through the family. There are many forms of CMT disease, including CMT1, CMT2, CMT3, CMT4, and CMTX. CMT1, caused by abnormalities in the myelin sheath, has three main types.
CMT1A is an autosomal dominant disease that results from a duplication of the gene on chromosome 17 that carries the instructions for producing the peripheral myelin protein-22 (PMP-22). The PMP-22 protein is a critical component of the myelin sheath. Overexpression of this gene causes the structure and function of the myelin sheath to be abnormal. Patients experience weakness and atrophy of the muscles of the lower legs beginning in adolescence; later they experience hand weakness and sensory loss.
CMT1B is an autosomal dominant disease caused by mutations in the gene that carries the instructions for manufacturing the myelin protein zero (P0), which is another critical component of the myelin sheath.
CMT2 results from abnormalities in the axon of the peripheral nerve cell rather than the myelin sheath. It is less common than CMT1.
CMT3 or Dejerine-Sottas disease is a severe demyelinating neuropathy that begins in infancy. Infants have severe muscle atrophy, weakness, and sensory problems
CMT4 comprises several different subtypes of autosomal recessive demyelinating motor and sensory neuropathies. Individuals with CMT4 generally develop symptoms of leg weakness in childhood and by adolescence they may not be able to walk.
CMTX is caused by a point mutation in the connexin-32 gene on the X chromosome. Males who inherit one mutated gene from their mothers show moderate to severe symptoms of the disease beginning in late childhood or adolescence. Females who inherit one mutated gene from one parent and one normal gene from the other parent may develop mild symptoms in adolescence or later or may not develop symptoms of the disease at all.
How is Charcot-Marie-Tooth disease diagnosed?
Diagnosis of CMT begins with a standard medical history, family history, and neurological examination. Individuals will be asked about the nature and duration of their symptoms and whether other family members have the disease. During the neurological examination a physician will look for evidence of muscle weakness in the individual’s arms, legs, hands, and feet, decreased muscle bulk, reduced tendon reflexes, and sensory loss. Doctors look for evidence of foot deformities, such as high arches, hammertoes, inverted heel, or flat feet. Other orthopedic problems, such as mild scoliosis or hip dysplasia, may also be present. A specific sign that may be found in people with CMT1 is nerve enlargement that may be felt or even seen through the skin. These enlarged nerves, called hypertrophic nerves, are caused by abnormally thickened myelin sheaths.
If CMT is suspected, the physician may order electrodiagnostic tests. This testing consists of two parts: nerve conduction studies and electromyography (EMG). During nerve conduction studies, electrodes are placed on the skin over a peripheral motor or sensory nerve. These electrodes produce a small electric shock that may cause mild discomfort. This electrical impulse stimulates sensory and motor nerves and provides quantifiable information that the doctor can use to arrive at a diagnosis. EMG involves inserting a needle electrode through the skin to measure the bioelectrical activity of muscles. Specific abnormalities in the readings signify axon degeneration. EMG may be useful in further characterizing the distribution and severity of peripheral nerve involvement.
Genetic testing is available for some types of CMT and results are usually enough to confirm a diagnosis. In addition, genetic counseling is available to assist individuals in understanding their condition and plan for the future.
If all the diagnostic work-up in inconclusive or genetic testing comes back negative, a neurologist may perform a nerve biopsy to confirm the diagnosis. A nerve biopsy involves removing a small piece of peripheral nerve through an incision in the skin. This is most often done by removing a piece of the nerve that runs down the calf of the leg. The nerve is then examined under a microscope.
The treatment of CMT:
There is no cure for CMT, but physical therapy, occupational therapy, braces and other orthopedic devices, and even orthopedic surgery can help individuals cope with the disabling symptoms of the disease. In addition, pain-killing drugs can be prescribed for individuals who have severe pain.
Physical and occupational therapy, the preferred treatment for CMT, involves muscle strength training, muscle and ligament stretching, stamina training, and moderate aerobic exercise. Most therapists recommend a specialized treatment program designed with the approval of the person’s physician to fit individual abilities and needs. Therapists also suggest entering into a treatment program early; muscle strengthening may delay or reduce muscle atrophy, so strength training is most useful if it begins before nerve degeneration and muscle weakness progress to the point of disability.
Stretching may prevent or reduce joint deformities that result from uneven muscle pull on bones. Exercises to help build stamina or increase endurance will help prevent the fatigue that results from performing everyday activities that require strength and mobility. Moderate aerobic activity can help to maintain cardiovascular fitness and overall health. Most therapists recommend low-impact or no-impact exercises, such as biking or swimming, rather than activities such as walking or jogging, which may put stress on fragile muscles and joints.
Many CMT patients require ankle braces and other orthopedic devices to maintain everyday mobility and prevent injury. Ankle braces can help prevent ankle sprains by providing support and stability during activities such as walking or climbing stairs. High-top shoes or boots can also provide support for weak ankles. Thumb splints can help with hand weakness and loss of fine motor skills. Assistive devices should be used before disability sets in because the devices may prevent muscle strain and reduce muscle weakening. Some individuals with CMT may decide to have orthopedic surgery to reverse foot and joint deformities.
The National Institute of Neurology Disorders and Stroke supports research on CMT and other peripheral neuropathies in an effort to learn how to better treat, prevent, and even cure these disorders.
“Spina bifida is one of the most common birth defects today and may be called by a number of other clinical names, such as spina bifida cystica and myelodysplasia, both of which are synonyms of ‘spina bifida’.”
Columbia Presbyterian Hospital – Orthopaedic Surgery
“It’s Halloween time and the flu season is here! Keeping hands clean by washing them with soap and water is one of the best ways to prevent the spread of germs. Everyone 6 months and older should get a flu vaccine each year for the best protection against influenza throughout flu season.”
CDC (center for disease control & prevention)
Go to striveforgoodhealth.com on Safety tips regarding halloween for kids.
“A full 70 percent of people say chocolate is their favorite Halloween treat, followed by candy corn (13 percent), chewy candy (6 percent) and gummy candy (5 percent).”
National Confection National Confectioners Association’s (NCA)
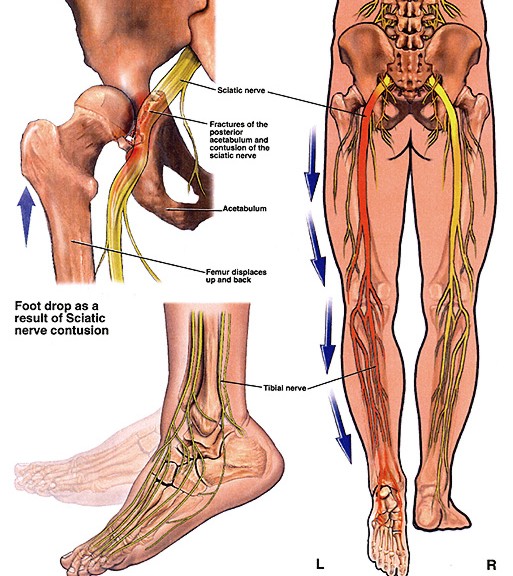
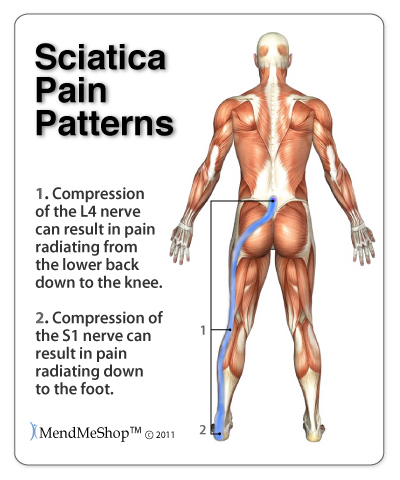
Sciatica is pain, tingling, or numbness produced by an irritation of the nerve roots that lead to the sciatica nerve. The sciatic nerve is formed by the nerve roots coming out of the spinal cord into the lower back. It goes down through the buttock, then its branches extend down the back of the leg to the ankle and foot. When something presses on the sciatica nerve, like a herniated disc, it presses on that nerve which causes the pain from the buttock that can radiate all the way down to the foot. The intensity of the pressure on the nerve and where its pressed decides if it goes to the foot or less. Other causes of sciatica nerve damage:
The most common cause -a bulging or ruptured disc in the spine pressing against the nerve roots that lead to the sciatic nerve.
-Sciatica Nerve Damage can be a symptom of other conditions that affect
*Narrowing of the spinal canal due to spinal stenosis. This spinal canal narrowing pinches on the sciatica nerve.
*Bone spurs-they are growths that are small forming along joints caused by arthritis.
*Simply injury (like a car accident or fall) causing nerve root compression=again the same result-pinching the sciatica nerve.
*Pregnancy-not as common as a cause as the others listed.
*Rarely but also tumors could cause the problem also.
What are the symptoms?
Symptoms of sciatica include pain that begins in your back or buttock and moves down your leg and may move into your foot.
*Weakness, tingling, or numbness in the leg may also occur.
*At times a inconsistent stabbing feeling or pricking feeling in the ankle or foot
*Sitting, standing for a long time, and movements that cause the spine to flex (such asexercises using the knee to chest) which may make symptoms worse.
*Walking, lying down, and movements that extend the spine (such as press-ups) may relieve symptoms.
How is sciatica diagnosed?
Sciatica is diagnosed with a medical history and physical exam. Sometimes x-rays and other tests such as magnetic resonance imaging (MRI) are done to help find the cause of the sciatica.
What are the Complications?
Although most people recover fully from sciatica, often without any specific treatment, sciatica can potentially cause permanent nerve damage. Seek immediate medical attention if you experience:
-Loss of feeling in the affected leg -Weakness in the affected leg
-Loss of bowel or bladder function
How is it treated?
In many cases, sciatica will improve and go away with time. Initial treatment usually focuses on medicines and exercises to relieve pain. You can help relieve pain by:
*Avoiding sitting (unless it is more comfortable than standing).
*Alternating lying down with short walks. Increase your walking distance as you are able to, without pain.
* Takingacetaminophen (tylenol) or Motrin (Ibuporfen) or Advil or Aleve (Naproxen). All are nonsteroidal anti-inflammatory drugs which decrease the swelling of the inflammation around the area or injury to the back which will decrease the pain. More inflammation=more pinching on the nerve.
*Using a heating pad on a low or medium setting for 15 to 20 minutes every 2 or 3 hours. Try a warm shower in place of one session with the heating pad. You can also buy single-use heat wraps that last up to 8 hours. You can also try an ice pack for 10 to 15 minutes every 2 to 3 hours. There is not strong evidence that either heat or ice will help, but you can try them to see if they help you.
*Additional treatment for sciatica depends on what is causing the nerve irritation. If your symptoms do not improve, your doctor may suggest physical therapy, injections of medicines such as steroids, stronger medicines such as muscle relaxants or opiates.
*Physical Therapy or chiropracter therapy or some form of therapy for 6 to 8 weeks.
* If the therapy is uneffective than the last resort in most cases is surgery that ranges from:
– laser surgery
– scrapping of the vertebrae pinching the nerve with leaving the rest of the vertebrae spacing the spinal cord in place or removing the vertebrae pinching the nerve and replacing it with cement (not cement we use for sidewalks that we know of). It’s natural to want to return to your regular activities as soon as possible after surgery, but a lot depends on the type of operation you get.
In two common methods, vertebroplasty and kyphoplasty, your surgeon makes a small cut in your back, which lets you recover faster. If you get spinal fusion surgery, the cut is larger, and it will take a longer time to heal.
-small endoscopic surgery that is microsurgery removing pieces of the vertebraepinching which has a test called a discogram (injecting a dye right into the injured disc and than a ultrasound of the area is done to show the surgeon the exact route he has to follow to cure the problem. The surgeon numbs the area that he will repair with the pt wide awake; he makes a incision about 2/10 of an inch, using the cat scan as a guide for his eyes inserting a scope inserting a grabber that goes in the scope removing disc fragments that are pressing on the nerves causing the pain. It takes about 30 minutes for this procedure with only a small bandage covering the incision followed with the patient leaving the hosp–ital in less than a few hours
*Other self-care treatments that may be helpful include:
-Cold packs. Initially, you may get relief from a cold pack placed on the painful area for up 20 minutes several times a day. Use an ice pack or a package of frozen peas wrapped in a clean towel.
-Hot packs. After two to three days, apply heat to the areas that hurt. Use hot packs, a heat lamp or a heating pad on the lowest setting. If you continue to have pain, try alternating warm and cold packs.
-Stretching. Stretching exercises for your low back can help you feel better and may help relieve nerve root compression. Avoid jerking, bouncing or twisting during the stretch and try to hold the stretch at least 30 seconds.
-Over-the-counter medications. Pain relievers such as ibuprofen (Advil, Motrin, others) and naproxen (Aleve) are sometimes helpful for sciatica.
References:
National Cancer Society
Web MD
Mayo Clinic
Dr. Bruce Hensel M.D. (chief medical editor channel 4)/Dr. David Ditsworth Surgeon – does back scoping -Robert Forrest Physical Therapy in Santa Monica, California.In this article
Michael Burgess (born 31 March 1946, is the Coroner of the Queen’s Household).

FLU FACTS:
-Both colds and flu usually last the same seven to 10 days, but flu can go three to four weeks; the flu virus may not still be there, but you have symptoms long after it has left. Allergy can last weeks or months.
-The winter flu epidemic will be coming around us again and in a given locality it reaches its peak in 2 to 3 weeks and lasts 5 to 6 weeks. Then is disappears as quickly as it arrived. The reason for this is not completely clear. The usual pattern is for a rise in the incidence of flu in children, which precedes an increase in the adult population.
-The flu virus can lead to serious complications, including bronchitis, viral or bacterial pneumonia and even death in elderly and chronically ill patients. Twenty thousand or more people die of the flu in the America each year. Know this that the frequency of human contact across the world and the highly infectious nature of the virus make this explanation difficult to accept. Moreover there is no evidence of persistent or latent infection with influenza viruses. In any case, this idea is not really very difficult from the notion that the virus circulates at a low level throughout the year and seizes its opportunity to cause an outbreak when conditions allow.
-Even harder to explain is why the flu disappears from a community when there are still a large number of people susceptible to infection. Than even harder than that is why flu is a winter disease, which is not fully understood or known. However, flu is spread largely by droplet (aerosol) infection from individuals with high viral level in their nasal and throat secretions, sneezing, and coughing on anyone close at hand. The aerosol droplets of the right size (thought to be about 1.5 micrometers in diameter) remain airborne and are breathed into the nose or lungs of the next victim.
-Situations in which people are crowded together are more commonly in cold or wet weather and so perhaps this contributes to spreading the flu at these times. It is interesting that in equatorial countries, flu occurs throughout the year, but is highest in the monsoon or rainy season. Enough about facts but onto logical thinking for when we or someone we know has it and what questions we might be asking ourselves.
LOGICAL QUESTIONS YOU MAY ASK YOURSELF:
Are the treatments for these illnesses the cold or the flu different? For any of these things, if it affects the nose or sinus, just rinsing with saline that gets the mucus and virus out is a first-line defense. It’s not the most pleasant thing to do, but it works very well. There are classes of medicines that can help the flu — Tamiflu and Relenza — antivirals that block viruses’ ability to reproduce and shorten the length and severity of the illness. But they have to be taken within 48 hours or the cat is proverbially out of the bag [because by then] the virus has done the most of its reproduction. For a cold or flu, rest and use decongestants and antihistamines, ibuprofen, acetaminophen, chicken soup and fluids. Zinc supposedly helps the body’s natural defenses work to their natural capacity and decrease the severity and length of a cold. Cells need zinc as a catalyst in their protective processes, so if you supply them with zinc, it helps them work more efficiently. You should also withhold iron supplements. Viruses use iron as part of their reproductive cycle, so depriving them of it blocks their dissemination. The majority of these infections are not bacterial and do not require [nor will they respond to] antibiotics. My rule of thumb is that a viral infection should go away in seven to 10 days. If symptoms persist after that, you’d consider if it’s bacteria like Strep or HaemophilusHYPERLINK “http://www.sciam.com/article.cfm?id=how-much-aids-vaccine-do” HYPERLINK “http://www.sciam.com/article.cfm?id=how-much-aids-vaccine-do”influenzae. Those bacteria cause illnesses that are longer lasting and need antibiotics for ranging 3 to 14 days, depending on the med used. Is that treatment approach the same for kids versus adults? In general, the same rules apply: Most children will have six to eight colds a year in their first three years of life, and most are viral. Adults have 3 or more a year. It’s very easy to test for strep and for that you should have a [positive] culture [before treating with antibiotics]. The principle behind that is knowing the organism the doctor will know what antibiotic to use to fight off the bacterial infection and you won’t build up antibodies from the antibiotic that you didn’t need in the first place if you are given the wrong antibiotic in the beginning. Are the strategies for avoiding cold and flu different? Avoidance is very similar: Strict hand washing, not sharing drinking cups or utensils, and avoiding direct contact with people who are sneezing. Their transmission is similar. As long as someone has a fever, they have the possibility to transmit infection. After they’ve had no fever for 24 hours, they’re not infectious anymore. The U.S. Centers for Disease Control and Prevention (CDC) now recommends that just about everyone get the flu shot: kids 6 months to 19 years of age, pregnant women, people 50 and up, and people of any age with compromised immune systems. Is the shot beneficial to anyone who gets it? Unless you have a contraindication, there’s no reason not to get it=PREVENTION. Contraindications include egg allergy (because the vaccine is grown from egg products), any vaccines within a last week or two, and active illness at the time of your vaccine.
The best to do is PREVENTION so you can avoid the cold or flu in its active phase or post phase, so doing the following will help prevent it:
Live a healthy lifestyle overall=Good dieting, living good healthy habits and maintaining exercise with rest daily or 2 to 3 times a week including get a vaccine yearly for the flu with maintaining good clean anti-infection habits like as simply as washing the hands as directed above.
If you need help in being given the knowledge in how routinely lose weight if not maintain your good weight, knowing what foods are lean to leaner to leanest out of the 4 food groups, understanding why portions of meals including exercise balanced with rest is so important, how all 4 interact with each other impacting your metabolism rate, and keeping a healthier body with a higher chance of increasing your immunity with fighting off simple colds to possibly the flu when near someone contaminated with the virus and making this a regular part not just a few months to a year but for life then you came to the right blog. This is provided through Dr. Anderson and myself as your health coach if you need one in where we help you get started on this goal in your life. You can order Dr. Anderson’s book “Dr. A’s healthy habits” that provides the information on foods to help you lose the excess of weight with so much more in learning about the body to diseases in prevention and Rx. Most important, you make all the choices. I needed to lose weight and lost what I wanted. So if you want to prevent getting the cold to the flu with so many other diseases and illnesses go to healthyusa.tsfl.com and join what I did for a starting help. Take a peek for no charge, no obligation and no hacking. I hope you have learned something new from my blog.
****Recommended is to check with your MD on any changes with diet or exercise especially if diagnosed already with disease or illness for your safety.****
References for Part 1,2, and 3 on the two bugs The FLU and The COLD:
1-Wikipedia “the free encyclopedia” 2013 website under the topic Influenza.
2-Kimberly Clark Professional website under the influenza.
3-Web MD under “COLD, FLU, COUGH CENTER” “Flu or cold symptoms?” Reviewed by Laura J. Martin MD November 01, 2011
4-2013 Novartis Consumer Health Inc. Triaminic “Fend off the Flu”
5-Scientific American “Why do we get the flu most often in the winter? Are viruses virulent in cold weather? December 15, 1997
Those bugs that are common in fall and winter are 2 Viruses =The COLD and THE FLU.
HOW THEY ARE DIFFERENT:
Both influenza and the common cold are viral respiratory infections (they affect the nose, throat, and lungs). Viruses are spread from person to person through airborne droplets (aerosols) that are sneezed out or coughed up by an infected person, direct contact is another form of spread with infected nasal secretions, or fomites (contaminated objects). Which of these routes is of primary importance has not been determined, however hand to hand and hand to surface to hand to contact seems of more importance than transmission. The viruses may survive for prolonged periods in the environment (over 18 hours for rhinoviruses in particular=a common virus for colds) and can be picked up by people’s hands and subsequently carried to their eyes or nose where infection occurs. In some cases, the viruses can be spread when a person touches an infected surface (e.g., doorknobs, countertops, telephones) and then touches his or her nose, mouth, or eyes. As such, these illnesses are most easily spread in crowded conditions such as schools.
The traditional folk theory that you can catch a cold in prolonged exposure to cold weather such as rain or winter settings is how the illness got its name. Some of the viruses that cause common colds are seasonal, occurring more frequently during cold or wet weather. The reason for the seasonality has not yet been fully determined. This may occur due to cold induced changes in the respiratory system, decreased immune response, and low humidity increasing viral transmission rates, perhaps due to dry air allowing small viral droplets to disperse farther, and stay in the air longer. It may be due to social factors, such as people spending more time indoors, as opposed to outdoors, exposing him or her “self” to an infected person, and specifically children at school. There is some controversy over the role of body cooling as a risk factor for the common cold; the majority of the evidence does suggest a result in greater susceptibility to infection.
The SIMPLE COMMON COLD:
The common cold (also known as nasopharyngitis, rhinopharyngitis, acute coryza, head cold) or simply a cold is a viral infection of the upper respiratory tract which primarily effects the nose. There are over 200 different known cold viruses, but most colds (30% up to 80%) are caused by rhinovirusesThis means you can pass the cold to others, so stay home and get some much-needed rest for yourself and not passing it on to others for the contagious period at least.
If cold symptoms do not seem to be improving after a week, you may have a bacterial infection, which means you may need antibiotics, which only kill bacterial infections not viral.
Sometimes you may mistake cold symptoms for allergic rhinitis (hay fever) or a sinus infection (bacterial). If cold symptoms begin quickly and are improving after a week, then it is usually a cold, not allergy. If your cold symptoms do not seem to be getting better after a week, check with your doctor to see if you have developed an allergy or inflammation or the sinuses (sinusitis).
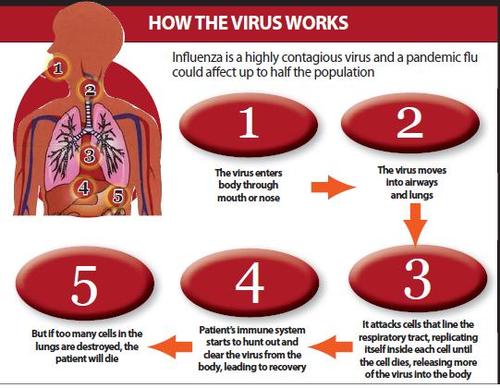
Influenza is commonly referred to as “the flu”, this is an infectious disease of birds and mammals caused by RNA viruses of the family Orthomyxoviridae, the influenza viruses. The most common sign or symptom are chills, fever, runny nose, coughing, aches and weakness to headache and sore throat. Although it is often confused with other influenza-like illnesses, especially the COMMON COLD, influenza is a more severe illness or disease caused by a different virus. Influenza nausea and vomiting, particularly in children but these symptoms are more common in the unrelated gastroenteritis, which is sometimes inaccurately referred to as “stomach flu” or “25 hour flu”. The flu can occasionally lead to pneumonia, either direct viral pneumonia or secondary bacterial pneumonia, even for persons who are usually very healthy. In particular it is a warning sign if a child or presumably an adult seems to be getting better and then relapses with a high fever as this relapse may be bacterial pneumonia. Another warning sign is if the person starts to have trouble breathing.
Each year, 10% to 20% of Canadians are stricken with influenza. Although most people recover fully, depending on the severity of the flu season, it can result in an average of 20,000 hospitalizations and approximately 4000 to 8000 deaths annually in Canada. Deaths due to the flu are found mostly among high-risk populations, such as those with other medical conditions (such as diabetes or cancer) or weakened immune systems, seniors, or very young children. There are 3 types of influenza viruses: A, B, and C. Type A influenza causes the most serious problems in humans and can be carried by humans or animals (wild birds are commonly the host carriers). It is more common for humans seem to carry the most with ailments with type A influenza. Type B Influenza is found in humans also. Type B flu may cause less severe reaction than A type flu virus but for the few for the many can still be at times extremely harmed. Influenza B viruses are not classified by subtype and do not cause pandemics at this time. Influenza type C also found in people but milder than type A or B. People don’t become very ill from this Type C Influenza and do not cause pandemics.
The common cold eventually fizzles, but the flu may be deadly. Some 200,000 people in the U.S. are hospitalized and 36,000 die each year from flu complications — and that pales in comparison to the flu pandemic of 1918 that claimed between 20 and 100 million lives.
“With 30,000 deaths and 200,000 hospitalizations from the seasonal flu, those numbers are certainly higher than what we’ve seen of the swine flu. Protecting yourself from both viruses is very important.”
Kristi Yamaguchi (born July 12, 1971) is an American figure skater. She was the 1992 Olympic Champion in ladies’ singles.
People infected with an influenza or cold virus become contagious 24 hours after the virus enters the body (often before symptoms appear). Adults remain infectious (can spread the virus to others) for about 6 days, and children remain infectious for up to 10 days. Factors that may increase the risk of catching a cold are fatigue, emotional stress, smoking, mid-phase of the menstrual cycle, and nasal allergies. Factors that do not increase the risk of catching a cold include cold body temperature (Example being out in the cold or enlarged tonsils). General health status and eating habits do in that they have impact on your immunity and “fight or flight” in fighting off infection as opposed to getting sick due to a healthy body overall.
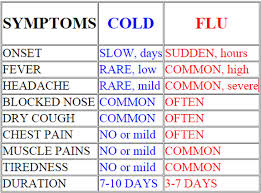
Watch for flu symptoms and in comparison here with the cold symptoms when trying to decipher what you have before going to the doctor. Signs and symptoms (S/S):
Flu s/s=High Fever lasting 3 to 4 days, prominent headache, general aches and pains which are often and severe, fatigue & weakness that lasts up to 2-3 wks., extreme exhaustion-early & prominent chest discomfort, cough-common & severe at times. *Note weakness and tiredness can last up to a few weeks with the Flu.
Cold S/S-Fever-rare, headache-rare, slight aches, mild fatigue if even present, extreme exhaustion (never occurs), Chest discomfort-mild if present, cough-moderate and hacking cough with sore throat sometimes present.
Common symptom: Stuffy nose is present, a common symptom for children is diarrhea and vomiting.
Regarding cold symptoms also be aware for these specifics, which include:
-Sore throat-usually is going away in about a day or three; nasal symptoms include runny nose and congestion to follow, along with a cough by the fourth or fifth day. Also, fever is uncommon in adults but a slight fever is possible. For children fever they can have with their cold. * -With the symptoms above you can also have the nose that teems with watery nasal secretions for the first few days later these become thicker and darker. Dark mucus is natural and does not mean you have developed a bacterial infection, such as a sinus infection.
**Know several hundred different viruses may cause your cold symptoms. A virus cannot be treated with an antibiotic since antibiotics can only fight off bacterial infections.**
Now let’s review what we know now, which is the common cold and the types of flu (Types A,B, and C), we know their symptoms (the cold versus the flu), we even know The Flu statistics of how many are affected yearly with what complications can arise, based on Part 1 and part of Part 2. The most important part of this article is letting my readers know or be aware of factors in prevention.
Let’s prepare ourselves in knowing factors for prevention of these 2 BUGS THE COLD and THE FLU (particularly) with knowing what to do when you or someone in the home has it.
The biggest factor in prevention of the COMMON COLD or THE FLU is living out your life utilizing great healthy habits and that would be washing your hands with soap and water often, especially: