
MS=Multiple Sclerosis is a long-lasting disease that can affect your brain, spinal cord, and the optic nerves in your eyes. It can cause problems with vision, balance, muscle control, and other basic body functions.
The effects are often different for everyone who has the disease. Some people have mild symptoms and don’t need treatment. Others will have trouble getting around and doing daily tasks.
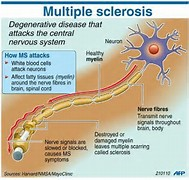
MS happens when your immune system attacks a fatty material called myelin, which wraps around your nerve fibers to protect them-an outer shell. Without this outer shell, your nerves become damaged. Scar tissue may form and transmission of signals from brain to the nerve endings with messages to do functions are obstructed in allowing the body to do functions.
Your nerves are the channels from the brain to the muscle it is going to. Understand that when your a fetus the brain first grows, and than the spinal cord continues to grow from the brain. They are both the same tissue. In MS this damage means your brain can’t send signals through your body correctly. Your nerves also don’t work as they should to help you move and feel. In multiple sclerosis (MS), the body’s immune system T cells attack the myelin sheath that protects the nerve fibers. The T cells either partially or completely strip the myelin off the fibers, leaving the nerves unprotected and uninsulated. Due to patches of the myelin sheath in your nerves unable to give messages so sensation and movement that the brain controls in the CNS is destroyed. Ending line making the mobility of the patient destroyed.
Multiple sclerosis (MS) is an unpredictable, often disabling disease of the central nervous system that disrupts the flow of information within the brain, and between the brain and nerves throughout the body.
It can be a challenge for doctors to diagnose multiple sclerosis (MS). There’s no one test that can definitely show if someone has it. And there are many conditions with symptoms that can seem like MS.
But a neurologist who specializes in treating the disease should be able to look into how you’re feeling and help you figure out if your symptoms mean you have MS or another problem.
The causes of MS – Multiple Sclerosis:
Doctors don’t know for sure what causes MS, but there are many things that seem to make the disease more likely.
People with certain genes may have higher chances of getting it.
Smoking also may raise the risk.
Some people may get MS after they’ve had a viral infection — like the Epstein-Barr virus or the human herpesvirus 6 — that makes their immune system stop working normally. The infection may trigger the disease or cause relapses. Scientists are studying the link between viruses and MS, but they don’t have a clear answer yet.
Some studies even suggest that vitamin D, which you can get from sunlight, may strengthen your immune system and protect you from MS.
Some people with higher chances of getting the disease move to sunnier regions seem to lower their risk; like my cousin from the NJ to South Carolina.
There are no specific tests for MS. Instead, a diagnosis of multiple sclerosis often relies on ruling out other conditions that might produce similar signs and symptoms, known as a differential diagnosis.
Diagnostic Tooling done for ruling out multiple sclerosis is:
*Imaging tests, like an MRI– to take a closer look at your brain. Magnetic resonance imaging, nuclear magnetic resonance imaging, or magnetic resonance tomography is a medical imaging technique used in radiology to image the anatomy and the physiological processes of the body in both health and disease. MRI scanners use strong magnetic fields, radio waves, and field gradients to form images of the body.
MRIs can reveal areas of MS (lesions) on your brain and spinal cord. You may receive an intravenous injection of a contrast material to highlight lesions that indicate your disease is in an active phase.
*Spinal taps, also called lumbar punctures, to check the fluid that runs through your spinal column When doctors do this test, they’re looking closely at the fluid in your spine, called cerebrospinal fluid, for higher levels of proteins and other substances that are signs of the disease. These can be helpful in diagnosing MS, but they’re not absolute proof of the condition. Your doctor can tell you if you need to have a spinal tap
*Electrical tests, called evoked potentials, to see if MS has affected your nerve pathways. Electrical tests of your nerves, called evoked potentials, can help doctors confirm if the condition has affected the parts of your brain that help you see, hear, and feel. Your doctor will place wires on your scalp to test your brain’s response as you watch a pattern on a video screen, hear a series of clicks, or get electrical pulses on your arm or leg.
The MD record the electrical signals produced by your nervous system in response to stimuli. An evoked potential test may use visual stimuli or electrical stimuli, in which you watch a moving visual pattern, or short electrical impulses are applied to nerves in your legs or arms. Electrodes measure how quickly the information travels down your nerve pathways.
*Blood tests. Tests to check for specific biomarkers associated with MS are currently under development and may also aid in diagnosing the disease.
*Evoked potential tests. Which record the electrical signals produced by your nervous system in response to stimuli. An evoked potential test may use visual stimuli or electrical stimuli. In these tests, you watch a moving visual pattern, or short electrical impulses are applied to nerves in your legs or arms. Electrodes measure how quickly the information travels down your nerve pathways.
Stayed tune to Part II tomorrow regarding signs/symptoms!

Updated 3/16/2023