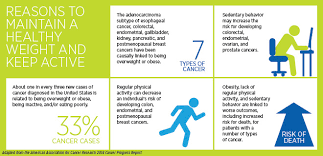

The problem with being overweight or obese, as measured by weight and height, is that it raises our risk of chronic diseases like diabetes and heart disease. But did you know that being obese can actually increase our risk of getting cancer and may even worsen our chances of surviving after a cancer diagnosis? In fact, the American Cancer Society Cancer Prevention Study II showed significant increases in cancer occurrence in people who are the most overweight. This link is stronger in some cancer types –including breast cancer after menopause, and cancers of the colon and rectum, pancreas, kidney, esophagus, and endometrium — and can be associated with a major increase in risk.
Being obese appears to be a problem for cancer survivors as well. Studies have shown worse survival for obese women with breast cancer; obese men with prostate cancer are more likely to have an aggressive form of cancer and it is more likely to come back after surgery. In light of this more recent data, the American Cancer Society recently released new healthy living guidelines for cancer survivors.
The relationship between body weight and cancer becomes more alarming when we consider just how many people in the United States are overweight or obese. Today, only 1/3 of adults are at a healthy body weight for their height. Another 1/3 are considered “overweight” and the remaining 1/3 are in the “obese” category. (About 17 % of children and adolescents are obese). These rates are 300% higher than in 1980.)
AMERICA wake up we have to turn this around for the better unless we don’t care about making this the home of the best country to live in a better one for all. We need to get healthier people especially if you have a condition, illness or disease that will let you but always get clearance by your doctor before making changes; to maintain your safety.
In a few years, obesity will replace smoking as the number one preventable cause of many common cancers, according to Professor Jeffrey M. P. Holly, Ph.D. With a grant from American Institute of Cancer Research (AICR), Professor Holly is examining how fatty acids affect the actions of insulin-like growth factors (IGFs), which may promote cancer. He is also looking at two phytochemicals that may interfere with the actions of IGFs and form part of a diet to prevent cancer.
Obesity results from a long-term energy imbalance that increases a person’s storage of fat and circulating levels of fatty acids. These higher levels of fatty acids can cause resistance to insulin, which is a hormone essential to regulating the body’s metabolism. Insulin resistance has been associated with the development of diabetes, heart disease and certain cancers. IGFs work in the body in a similar way to insulin. For a long time, Professor Holly, a Clinical Sciences Professor at the University of Bristol, U.K., has studied how these similar substances affect metabolic conditions such as diabetes. But for the past few years – as more recent research has shown that IGFs may be an important risk factor for colon, prostate and premenopausal breast cancer – he has looked at how obesity increases cancer risk through effects upon secretion and action of insulin and IGFs. Recently, he and his research colleagues realized that “no one had looked at what effect eating fatty foods has on IGFs, especially now that we know that IGFs may be related to nutrition-dependent cancers.” Focus on Two Fatty Acids With funding from AICR (American Institute of Cancer Research), Dr. Holly and his research team have begun a series of experiments on malignant and healthy breast cells. They will see what impact the most abundant circulating fatty acids – palmitate and oleate – have on these cells by way of the production and activity of IGFs. Palmitate is a saturated fatty acid, while oleate is an unsaturated fatty acid. “We’re looking at three aspects of these cells’ functions: their metabolism, their growth and their survival,” said Dr. Holly. “For cancer to develop, cell growth and survival are critical.” Normally, when a cell becomes damaged, it is genetically programmed to die prematurely. This process is called apoptosis. IGFs, however, interfere with apoptosis. “IGFs are known to be the most potent, powerful signal in the body telling the cells not to commit suicide,” said Dr. Holly. “If there is too strong an IGF signal in the body, damaged cells may live and grow into tumors. That’s the most plausible link between high IGF levels and high rates of some cancers.” Palmitate and oleate are known to affect insulin-related metabolic conditions differently. Palmitate appears to make the body more resistant to insulin, while oleate reduces resistance to insulin. But it is too early in Dr. Holly’s two-year experiment to know how the two fatty acids affect actions of IGF. The Flavonoid Effect As part of his AICR-funded project, Professor Holly will see whether two flavonoids – epigallocatechin-3-gallate (EGCG), found in green tea, and luteolin, found in olive oil – affect the growth of both the malignant and healthy cells. He will expose the cells to the flavonoids under various conditions to determine how strong their influence is. Professor Holly chose to examine flavonoids as possible cancer-preventive agents in this obesity-related study because the fat we consume is not our body’s only source of fatty acids. Our bodies have the ability to make some of their own fatty acids when needed. In fact, certain cancers, like breast cancer, tend to make huge amounts in order to maintain their growth rate. Flavonoids are known to inhibit this process. This inhibition may partly explain why a diet high in vegetables and fruits protects against cancer in many studies. Professor Holly suggests that the benefits of eating a lot of vegetables and fruits may be negated by a high-fat diet, because there would be a surplus of fatty acids to feed cells. Although his research project is in a preliminary stage, the investigation is important because it could show how certain diets, especially those low in fat, can help prevent cancer. His study may also demonstrate that some diets may be more beneficial for people undergoing cancer treatment. “Most treatments, like radiation therapy and chemotherapy, encourage cancer cells to die,” said Dr. Holly. “If we can manipulate the environment within the body to make cell death easier, these therapies may be more effective. One way to do this may be to turn off some of the signals from IGFs that encourage malignant cells to survive.”
Obesity is associated with increased risks of the following cancer types,&possibly others as well:
Esophagus/Pancreas/Colon and rectum/Breast (after menopause) /Endometrium (lining of the uterus)/Kidney/Thyroid/Gallbladder
One study, using NCI Surveillance, Epidemiology, and End Results (SEER) data, estimated that in 2007 in the United States, about 34,000 new cases of cancer in men (4 percent) and 50,500 in women (7 percent) were due to obesity. The percentage of cases attributed to obesity varied widely for different cancer types but was as high as 40 percent for some cancers, particularly endometrial cancer and esophageal adenocarcinoma.
A projection of the future health and economic burden of obesity in 2030 estimated that continuation of existing trends in obesity will lead to about 500,000 additional cases of cancer in the United States by 2030. This analysis also found that if every adult reduced their BMI by 1 percent, which would be equivalent to a weight loss of roughly 1 kg (or 2.2 lbs) for an adult of average weight, this would prevent the increase in the number of cancer cases and actually result in the avoidance of about 100,000 new cases of cancer.
***Come back tomorrow for Part 2 and see case studies that support this article with how to try to prevent this through living healthier habits, healthy dieting, and balancing rest with exercise. You may just want to take a peek, hope I see you tomorrow.***