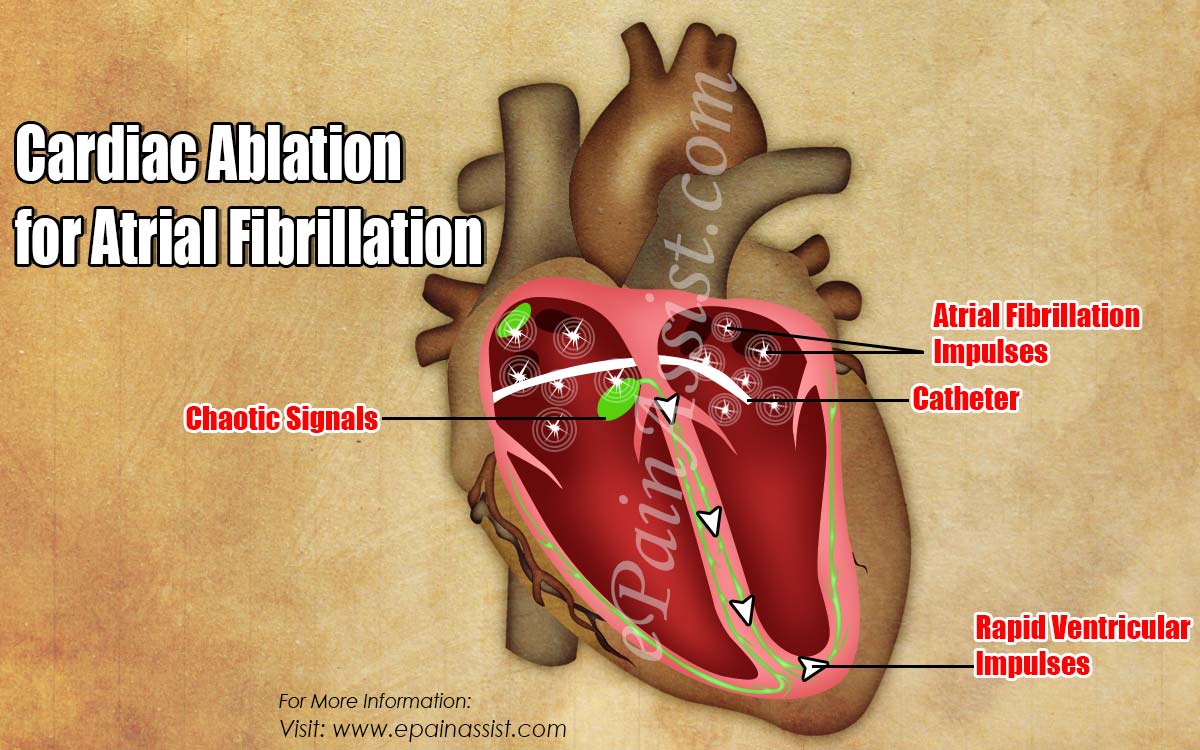
In this cardiac ablation, follow the pointer to the yellow spot in upper R atrium, is where the this ends procedure ends.
In this cardiac ablation, follow the pointer to the yellow spot in upper R atrium, is where the this ends procedure ends.
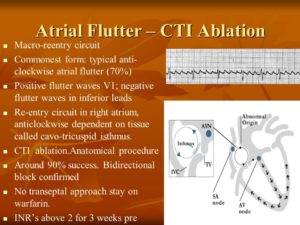
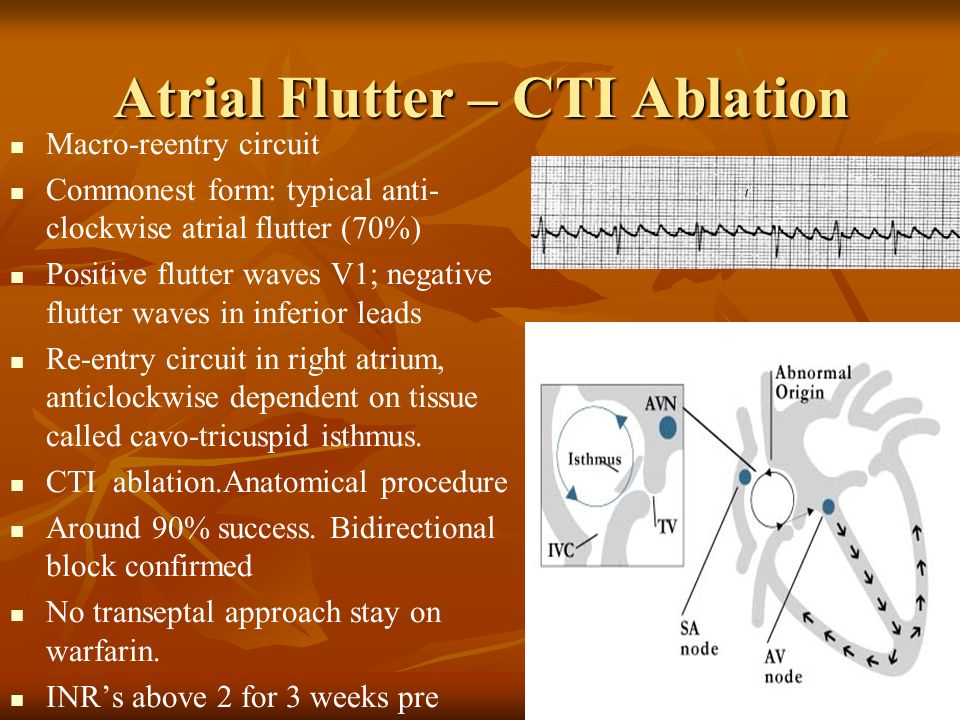
Macro-reentry circuit. Commonest form: typical anti-clockwise atrial flutter (70%) Positive flutter waves V1; negative flutter waves in inferior leads. Re-entry circuit in right atrium, anticlockwise dependent on tissue called cavo-tricuspid isthmus. CTI ablation.Anatomical procedure. Around 90% success. Bidirectional block confirmed. No transeptal approach stay on warfarin. INR’s above 2 for 3 weeks pre.
Ablation is a procedure used to treat abnormal heart rhythms, or arrhythmias. The type of arrhythmia and the presence of other heart disease will determine whether ablation can be performed surgically or non-surgically but ending line its removing of or destruction of tissue.
The term “arrhythmia” refers to any change from the normal sequence of electrical impulses. The electrical impulses may happen too fast, too slowly, or erratically – causing the heart to beat too fast, too slowly, or erratically. When the heart doesn’t beat properly, it can’t pump blood effectively. When the heart doesn’t pump blood effectively, the lungs, brain and all other organs can’t work properly and may shut down or be damaged.
Electrical signals control the pump=HEART
The heart beat (contraction) begins when an electrical impulse from the sinoatrial node (also called the SA node or sinus node) moves through it. The SA node is sometimes referred to as the heart’s “natural pacemaker” because it initiates impulses for the heartbeat.
The normal electrical sequence begins in the right atrium and spreads throughout the atria to the atrioventricular (AV) node. From the AV node, electrical impulses travel down a group of specialized fibers called the His-Purkinje system to all parts of the ventricles.
This exact route must be followed for the heart to pump properly. As long as the electrical impulse is transmitted normally, the heart pumps and beats at a regular pace. In an adult, a normal heart beats 60 to 100 times a minute.
Electrocardiography (ECG or EKG) is a painless, non-invasive procedure that records the heart’s electrical activity and can help diagnose arrhythmias.
Abnormal heart rhythms (arrhythmias)
Arrhythmias are abnormal beats. The term “arrhythmia” refers to any change from the normal sequence of electrical impulses, causing abnormal heart rhythms. Arrhythmias may be completely harmless or life-threatening.
Some arrhythmias are so brief (for example, a temporary pause or premature beat) that the overall heart rate or rhythm isn’t greatly affected. But if arrhythmias last longer, they may cause the heart rate to be too slow or too fast or the heart rhythm to be erratic – so the heart pumps less effectively.
- A fast heart rate (in adults, more than 100 beats per minute) is called tachycardia.
- A slow heart rate (less than 60 beats per minute) is referred to as bradycardia.
Causes
- Normally, the heart’s most rapidly firing cells are in the sinus (or sinoatrial or SA) node, making that area a natural pacemaker.
- Under some conditions almost all heart tissue can start an impulse of the type that can generate a heartbeat. Cells in the heart’s conduction system can fire automatically and start electrical activity. This activity can interrupt the normal order of the heart’s pumping activity.
- Secondary pacemakers elsewhere in the heart provide a “back-up” rhythm when the sinus node doesn’t work properly or when impulses are blocked somewhere in the conduction system.
An arrhythmia occurs when:
- The heart’s natural pacemaker develops an abnormal rate or rhythm.
- The normal conduction pathway is interrupted.
- Another part of the heart takes over as pacemaker.
Non-surgical ablation, used for many types of arrhythmias, is performed in a special lab called the electrophysiology (EP) laboratory. During this non-surgical procedure a catheter is inserted into a specific area of the heart. A special machine directs energy through the catheter to small areas of the heart muscle that causes the abnormal heart rhythm. This energy “disconnects” the source of the abnormal rhythm from the rest of the heart. It can also be used to disconnect the electrical pathway between the upper chambers (atria) and the lower chambers (ventricles) of the heart.
Surgical ablation procedures used for treating atrial fibrillation can be “minimally invasive” or traditional “open” surgery and may be combined with other surgical therapies such as bypass surgery, valve repair, or valve replacement. Surgical ablation procedures include:
- The Maze procedure. During this traditional open-heart surgical procedure, the surgeon makes small cuts in the heart to interrupt the conduction of abnormal impulses and to direct normal sinus impulses to travel to the atrioventricular node (AV node) as they normally should. When the heart heals, scar tissue forms and the abnormal electrical impulses are blocked from traveling through the heart.
- Minimally invasive surgical ablation. Unlike traditional heart surgery, there is no large chest wall incision and the heart is not stopped. These techniques utilize smaller incisions and endoscopes (small, lighted instruments that contain a camera).
- The modified Maze procedure. The surgeon uses a special catheter to deliver energy that creates controlled lesions on the heart and ultimately scar tissue. This scar tissue blocks the abnormal electrical impulses from being conducted through the heart and promotes the normal conduction of impulses through the proper pathway. One of four energy sources may be used to create the scars: radiofrequency, microwave, laser, or cryothermy (cold temperatures). The modified Maze procedure involves a single incision in the left atrium.
How effective and safe is this procedure?
Radiofrequency ablation has a success rate of over 90 percent, a low risk of complications and the patient can resume normal activities in a few days. It causes little or no discomfort and is done under mild sedation with local anesthesia. For these reasons, it’s now widely used and is the preferred treatment for many types of rapid heartbeats.
What are the risks of catheter ablation?
There are few risks. Fewer than 5 percent of people who have the procedure develop any problems. The most common problems result from the use of the catheters – long, thin tubes doctors insert into your arteries or veins. Inserting the tubes can occasionally damage your blood vessel or cause bleeding or infection. These problems are rare.