“Common treatments for stage IV bone cancer: In stage IV bone cancer,surgery is often the recommended course of treatment.Radiation, chemotherapy and targeted therapies may also be recommended.”
Cancer Treatment of America
“Common treatments for stage IV bone cancer: In stage IV bone cancer,surgery is often the recommended course of treatment.Radiation, chemotherapy and targeted therapies may also be recommended.”
Cancer Treatment of America
“The foods you eat, especially foods high in antioxidants, can help ward off dementia and improve your brain health. As Stony Brook University registered dietitian Stephanie May tells students, choosing colorful fruits and vegetables – and avoiding processed foods – will fuel you for success.”
U.S. Health News
There’s no denying that as we age chronologically, our body ages right along with us. But research is showing that you can increase your chances of maintaining a healthy brain well into your old age if you add these “smart” foods to your daily eating regimen.
Blueberries.
“Brainberries” is what Steven Pratt, MD, author of Superfoods Rx: Fourteen Foods Proven to Change Your Life, calls these tasty fruits. Pratt, who is also on staff at Scripps Memorial Hospital in La Jolla, Calif., says that in animal studies researchers have found that blueberries help protect the brain from oxidative stress and may reduce the effects of age-related conditions such as
Alzheimer’s disease or dementia. Studies have also shown that diets rich in blueberries significantly improved both the learning capacity and motor skills of aging rats, making them mentally equivalent to much younger rats. Ann Kulze, MD, author of Dr. Ann’s 10-Step Diet: A Simple Plan for Permanent Weight Loss & Lifelong Vitality, recommends adding at least 1 cup of blueberries a day in any form — fresh, frozen, or freeze-dried.
Wild salmon.
Deep-water fish, such as salmon, are rich in omega-3 essential fatty acids, which are essential for brain function, says Kulze. Both she and Pratt recommend wild salmon for its “cleanliness” and the fact that it is in plentiful supply. Omega-3s also contain anti-inflammatory substances. Other oily fish that provide the benefits of omega-3s are sardines and herring, says Kulze; she recommends a 4-ounce serving, two to three times a week.
Nuts and seeds.
Nuts and seeds are good sources of vitamin E, says Pratt, explaining that higher levels of vitamin E correspond with less cognitive decline as you get older. Add an ounce a day of walnuts, hazelnuts, Brazil nuts, filberts, almonds, cashews, peanuts, sunflower seeds, sesame seeds, flax seed, and unhydrogenated nut butters such as peanut butter, almond butter, and tahini. Raw or roasted doesn’t matter, although if you’re on a sodium-restricted diet, buy unsalted nuts.
Avocados.
Avocados are almost as good as blueberries in promoting brain health, says Pratt. “I don’t think the avocado gets its due,” agrees Kulze. True, the avocado is a fatty fruit, but, says Kulze, it’s a monounsaturated fat, which contributes to healthy blood flow. “And healthy blood flow means a healthy brain,” she says. Avocados also lower blood pressure, says Pratt, and as hypertension is a risk factor for the decline in cognitive abilities, a lower blood pressure should promote brain health. Avocados are high in calories, however, so Kulze suggests adding just 1/4 to 1/2 of an avocado to one daily meal as a side dish.
Whole grains.
Whole grains, such as oatmeal, whole-grain breads, and brown rice can reduce the risk for heart disease. “Every organ in the body is dependent on blood flow,” says Pratt. “If you promote cardiovascular health, you’re promoting good flow to the organ system, which includes the brain.” While wheat germ is not technically a whole grain, it also goes on Kulze’s “superfoods” list because in addition to fiber, it has vitamin E and some omega-3s. Kulze suggests 1/2 cup of whole-grain cereal, 1 slice of bread two-thee times day, or 2 tablespoons of wheat germ a day.
Beans.
Beans are “under-recognized” and “economical,” says Kulze. They also stabilize glucose (blood sugar) levels. The brain is dependent on glucose for fuel, Kulze explains, and since it can’t store the glucose, it relies on a steady stream of energy — which beans can provide. Any beans will do, says Kulze, but she is especially partial to lentils and black beans and recommends 1/2 cup every day.
Pomegranate juice.
Pomegranate juice (you can eat the fruit itself but with its many tiny seeds, it’s not nearly as convenient) offers potent antioxidant benefits, says Kulze, which protect the brain from the damage of free radicals. “Probably no part of the body is more sensitive to the damage from free radicals as the brain,” says board-certified neurologist David Perlmutter, MD, author of The Better Brain Book. Citrus fruits and colorful vegetables are also high on Perlmutter’s list of “brainy” foods because of their antioxidant properties — “the more colorful the better,” he says. Because pomegranate juice has added sugar (to counteract its natural tartness), you don’t want to go overboard, says Kulze; she recommends approximately 2 ounces a day, diluted with spring water or seltzer.
Freshly brewed tea.
Two to three cups a day of freshly brewed tea — hot or iced — contains a modest amount of caffeine which, when used “judiciously,” says Kulze — can boost brain power by enhancing memory, focus, and mood. Tea also has potent antioxidants, especially the class known as catechines, which promotes healthy blood flow. Bottled or powdered teas don’t do the trick, however, says Kulze. “It has to be freshly brewed.” Tea bags do count, however.
Dark chocolate.
Let’s end with the good stuff and my favorite desert. Dark chocolate has powerful antioxidant properties, contains several natural stimulants, including caffeine, which enhance focus and concentration, and stimulates the production of endorphins, which helps improve mood. One-half ounce to 1 ounce a day will provide all the benefits you need, says Kulze. This is one “superfood” where more is not better. “You have to do this one in moderation,” says Kulze.
Lastly the prevention of diseases that can impact all organs including our brain. With obesity comes the risk of heart disease, diabetes II, that can lead into further problems down the road with other systems of the human body. To get on prevention check if your body mass index is in the range it should be and if your not sure check online BMI where it is for free. If you need assistance with a good diet plan but more importantly knowing how to get in a regular routine of living a healthy life through diet, habits, balancing rest with exercise than you have come to the right site. For no fee, no donation, no hacking go to healthyusa.tsfl.com and take a peek at what we offer which is at such a reasonable price. We provide more of a reachable goal for you with having Dr. Anderson through access of his book “Dr. A’s healthy habits” with a personal coach and the foods to eat while your dieting. If you have any questions or set backs and need to converse with someone that’s what your personal coach is there for; we provide support. Take a peek go to healthusa.tsfl.com and you may just like what you see. Join me and so many others in attempting to reach the goal of getting back in the right weight for our height. I hope to hear from you.
“In the United States, the percentage of children and adolescents affected by obesity has more than tripled since the 1970s.1 Data from 2015-2016 show that nearly 1 in 5 school age children and young people (6 to 19 years) in the United States has obesity.“
CDC Centers for Disease Control and Prevention


Dupuytren’s (du-pwe-TRANZ) contracture is a hand deformity that usually develops over years. The condition affects a layer of tissue that lies under the skin of your palm. This is a condition that affects the fascia—the fibrous layer of tissue that lies underneath the skin in the palm and fingers. In patients with Dupuytren’s, the fascia thickens, then tightens over time. This causes the fingers to be pulled inward, towards the palm, resulting in what is known as a “Dupuytren’s contracture.” Knots of tissue form under the skin — eventually creating a thick cord that can pull one or more fingers into a bent position. This is why, the fascia is a layer of tissue that helps to anchor and stabilize the skin on the palm side of the hand. Without the fascia, the skin on your palm would be as loose and moveable as the skin on the back of your hand. In patients with Dupuytren’s disease, this palmar fascia slowly begins to thicken, then tighten. As Dupuytren’s progresses, bands of fascia in the palm develop into thick cords that can tether one or more fingers and the thumb into a bent position. This is called a “Dupuytren’s contracture.” Although the cords in the palm may look like tendons, the tendons are not involved in Dupuytren’s.
This occurs most often in older men of Northern European descent.
The cause of Dupuytren’s disease is not completely known, but most evidence points towards genetics as having the most important role.
There are anecdotal reports of Dupuytren’s emerging or worsening after a patient experiences an injury or an open wound (including surgery) to his or her hand; however, there is no good evidence to support this. There is also no compelling evidence to suggest that it is caused by overuse of the hand.
This occurs most often in older men of Northern European descent.
The cause of Dupuytren’s disease is not completely known, but most evidence points towards genetics as having the most important role.
There are anecdotal reports of Dupuytren’s emerging or worsening after a patient experiences an injury or an open wound (including surgery) to his or her hand; however, there is no good evidence to support this. There is also no compelling evidence to suggest that it is caused by overuse of the hand.
Nodules. You may develop one or more small lumps, or nodules, the nodules may feel tender but, over time, this tenderness usually goes away. There can be “pitting” or deep indentation of the skin near the nodules.
Cords. The nodules may thicken & contract=the formation of dense and tough cords of tissue under the skin. These cords can restrict or tether the fingers and thumb from straightening or from spreading apart.
Contractures. The tissue under the skin tightens, one or more of your fingers may be pulled toward your palm and may be restricted from spreading apart. The ring and little fingers are most commonly affected, but any or all of the fingers can be involved, even the thumb.
As the bend in your finger increases, it may be hard to straighten it fully. It may be difficult to grasp large objects, put your hand in your pocket, or perform other simple activities.
In most cases, doctors can diagnose Dupuytren’s contracture by the look and feel of your hands. Other tests are rarely necessary. Your doctor will compare your hands to each other and check for puckering on the skin of your palms. He or she will also press on parts of your hands and fingers to check for toughened knots or bands of tissue. Your doctor also might check to see if you can put your hand flat on a tabletop or other flat surface. Not being able to fully flatten your fingers indicates you have Dupuytren’s contracture.
A number of treatments are available to slow the progression of Dupuytren’s contracture and relieve symptoms.
Know in most cases a Dupuytren’s contracture progresses very slowly, over a period of years, and may remain mild enough such that no treatment is needed. In moderate or severe cases, however, the condition makes it difficult to straighten the involved digits. When this happens, treatment may be needed to help reduce the contracture and improve motion in the affected fingers. Typically, as a contracture worsens, the involvement of the fascia becomes more severe and treatment is less likely to result in a full correction.
Currently, there is no cure for Dupuytren’s; however, the condition is not dangerous.
Although it varies from patient to patient, Dupuytren’s usually progresses very slowly and may not become troublesome for many years. In fact, for some patients, the condition may never progress beyond developing lumps in the palm.
If the condition progresses, your doctor may first recommend nonsurgical treatment to help slow the disease.
Steroid injection. Corticosteroids are powerful anti-inflammatory medications that can be injected into a painful nodule. In some cases, a corticosteroid injection may slow the progression of a contracture. The effectiveness of a steroid injection varies from patient to patient.
Splinting. Splinting is not known to prevent the progression of a finger contracture. Forceful stretching of the contracted finger may not be helpful and, in fact, could cause an injury to the finger or hand.
Splinting may be used after surgery for Dupuytren’s contracture to protect the surgical site; however, it is not known if it reduces the risk of recurrent contracture or tightening of the healing wound.
If the contracture interferes with hand function, your doctor may recommend surgical treatment. The goal of surgery is to reduce the contracture and improve motion in the affected fingers.
There is no known cure for Dupuytren’s contracture; however, surgery is intended to “set back the clock” by reducing the restricting effect of the cords by either disrupting or removing them. Unfortunately, the healing tissues will form with the same potential to develop cords in the future—but the gains in hand function can still be substantial.
The surgical procedures most commonly performed for Dupuytren’s contracture are:
Your doctor will talk with you about which procedure is best in your case.
Fasciotomy. In this procedure, your doctor will make an incision in your palm and then divide the thickened cord(s) of tissue. Although the cord itself is not removed, dividing it helps to decrease the contracture and increase movement of the affected finger.
Fasciotomy is performed using a local anesthetic that numbs just your hand without putting you to sleep. After the procedure, your wound will be left open and allowed to heal gradually. You will have to wear a splint during your recovery.

“Parents who delay or skip childhood vaccinations even when kids have no medical reasons are contributing to U.S. outbreaks of measles and whooping cough.”
Michigan Health Lab

There are many reasons parents give for delaying a vaccination, from “My baby cries when she gets the shot,” to “My child is too young to get so many vaccines.” More important than all of these excuses is one simple fact: A child’s immune system is more vulnerable without vaccinations. And if it weren’t for vaccinations, many children could become seriously ill or even die from diseases such as measles, mumps and whooping cough.
We live in an increasingly global world, with increased risks around every corner. Travelers entering into New York create an even greater risk of exposure. On a regular basis there is a new report regarding a disease outbreak somewhere in the world – including in the United States and New York State. The Centers for Disease Control and Prevention reports outbreaks around the world and provides health information for travel to more than 200 international destinations. (cdc.gov) From mumps, to pertussis to the measles, diseases once thought to be eradicated are coming back because people are not being vaccinated as they once were. If you think tears from a needle are hard to watch, imagine the suffering your child will experience if he or she contracts a serious disease that could have been prevented.
While misinformation in the media has led many parents to delay vaccinations as a result of either Dr. Andrew Wakefield’s false claims about autism or Dr. Bob’s Alternative Schedule (aap.org), many diseases have begun to reemerge among children around the world. Don’t let your child become a statistic — make sure they get all the recommended vaccinations. And if you’re worried about autism, visit “The Truth About Autism.”
Yes there are side effects to vaccinations but the odds are slim and the reason for the vaccinations in childhood including adulthood outweighs the possible risk for side effects. I have been a RN 31 years and have received the MMR (measles, mumps, and rubella) every 10 years, flu every year, & pneumonia every 5 years and have never gotten a side effect from them.
The threat of death by disease isn’t the only medical consequence of skipping vaccinations. An unvaccinated child faces lifelong differences that could potentially put him or her at risk. Every time you call 911, ride in an ambulance, go to the doctor or visit the hospital emergency room, you must alert medical personnel of your child’s vaccination status so he or she receives distinctive treatment. Because unvaccinated children can require treatment that is out of the ordinary, medical staff may be less familiar, and less experienced, with the procedures required to appropriately treat your child.
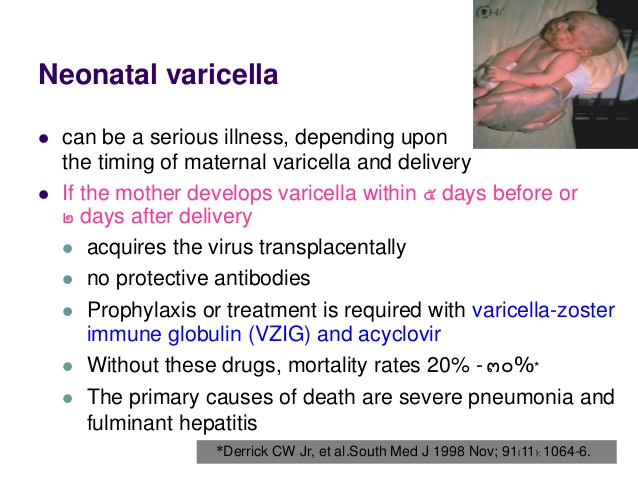
Women who are pregnant but not vaccinated can be vulnerable to diseases that may complicate their pregnancy. A pregnant woman who contracts rubella in the first trimester may have a baby with congenital rubella syndrome (CRS), which can cause heart defects, developmental delays and deafness.
People who choose not to vaccinate their children also put others at risk if their child isn’t vaccinated and becomes ill. Special groups of people cannot be vaccinated, including those with compromised immune systems (e.g. those with leukemia or other cancers). These people rely on the general public being vaccinated so their risk of exposure is reduced.
There are also social implications of not vaccinating your child — from exclusion to quarantine. If sick or exposed to disease, your child may need to be isolated from others, including family. If there is an outbreak in your community, you may be asked to take your child out of school and other organized activities, causing your child to miss school and special events. Your child’s illness or inability to go about their daily activities also may impact your work and household income. For more information on vaccination requirements for schools in the state of New York, see New York State Immunization Requirements for School Entrance/Attendance (PDF, 71KB, 2pg.).
Everyone 6 months and older should get a seasonal flu vaccine every year. It’s important to reiterate that every year the flu remains a threat, and every year children still die as a result of having the flu. One of those children was Joseph Marotta. At 5 years old, Joseph contracted the flu. Less than 10 days after contracting the flu, Joseph died. His parents, along with other members of Families Fighting Flu (familiesfightingflu.org), are strong advocates for annual flu vaccines and encourage all families to get vaccinated. It’s important that everyone 6 months and older receives an annual flu vaccine. Every year a flu vaccine is skipped, your child is at risk.
“As a result, many parents are inundated with horror stories of vaccine dangers, all designed to eat away at them emotionally while the medical and scientific communities have mounted their characteristic response by sharing the facts, the data, and all of the reliable peer-reviewed and well-cited research to show that vaccines are safe and effective. ”
U.S. National Library of Medicine/National Institutes of Health
“Most cases of cough are temporary. But even a short-term cough can be a sign of a bigger health issue that needs to be addressed by a doctor. Here’s how to narrow down the possible culprits—from asthma to pneumonia to whooping cough says Peter Dicpinigaitis, MD, director of the Montefiore Cough Center and professor of clinical medicine at Albert Einstein College of Medicine in New York City.”
Fox News.

The cough reflex is one of humans’ most vital defenses, highly effective in clearing secretions and preventing foreign materials from entering the lower respiratory tract. However, when a pathological cough persists without serving any useful purpose, it can be highly irritating and disruptive, causing significant sleep disturbance, chest pain, urinary incontinence, frustration, anger, and depression. “It’s easy to underestimate the tremendous quality of life issue that cough is, not only for the patient but for the family. Some of our patients have been coughing every single day for ten, twenty, even thirty years,” founded at the Montefiore Cough Center, one of the few specialty cough centers in the United States.
The Montifiore Cough Center found the following information via there research:
Despite the prevalence of cough, researchers have yet to fully understand its mechanism and relationship with the brain. Stimulation of the vagus—a cranial nerve with motor function in the larynx, esophagus, lower respiratory tract, and ear—can stimulate the cough reflex. The transient receptor potential vanilloid (TRPV1) receptor, a sensory nerve channel known as a “cough receptor,” induces the reflex when stimulated by irritants such as capsaicin (derived from red chili peppers), hydrogen, heat, low pH, certain enzymes, and anandamide (a naturally occurring, euphoria-inducing brain neurotransmitter).
The cough mystery presents a particular challenge to those who attempt to diagnose and treat it. Physicians need to maintain the protective cough, an important barrier reflex that prevents complications like bronchitis, pneumonia, and lung collapse, but eliminate the maladaptive cough. To do this successfully, the cough’s underlying etiology must be identified and addressed.
Manypatients cough due to post-nasal drip, or upper airway cough syndrome (UACS). UACS is often treated with a combination of a first-generation decongestant /antihistamine and other nasal corticosteroids, nasal ipratropium bromide, or nasal cromolyn. Newer generation, non-sedating antihistamines such as Claritin, Zyrtec, and Allegra, which circumvent drowsiness because they don’t pass the blood-brain barrier, are ineffective for treating UACS-associated cough.
Asthma, whether “cough-variant” (where cough is the sole or predominant symptom) or “classic” (with symptoms including wheezing) is the second most common cause of chronic cough, found in 24-29% of patients at Montefiore. Coughing inflames the sensory afferent nerves (those that carry messages from receptors to the central nervous system). Leukotrienes, lipid mediators whose production also generates histamines, are thought to contribute to the inflammation. Asthma therapy (usually a combination of inhaled bronchodilators and steroids) can take up to eight weeks to show improvement. An oral leukotriene receptor antagonist known as zafirlukast has in some cases been more effective than steroids in reducing asthma-associated cough, possibly because it more effectively suppresses the interaction of eosinophils (white blood cells that fight concomitant infection during asthmatic reaction) with cough receptors. Non-asthmatic eosinophilic bronchitis, a condition characterized by chronic cough without the airway remodeling common to asthma, is often misdiagnosed as cough-variant asthma because it responds similarly to inhaled corticosteroids.
Gastroesophageal reflux disease (GERD) is among the most common etiologies of cough, and perhaps the most difficult to diagnose. Most patients with reflux-associated cough have no other symptoms of GERD, though the characteristic heartburn, nausea, and regurgitation may subsequently appear. The standard GI workup for GERD—endoscopy, barium esophagram, prolonged esophageal acid monitoring, and impedance monitoring—may not detect mild acid exposure, brief reflux events, rapid esophageal clearance, and distal or “high” reflux. “You might send your patient for a full GI workup and receive test results that are unremarkable, but that patient’s reflux still causes an incredibly life-jarring cough”.
Chronic cough can also result from laryngopharyngeal reflux (LPR), a subtype of GERD in which reflux reaches the upper airways. People with LPR often cough when eating, drinking, laughing, talking on the telephone, or getting up in the morning, and may experience hoarseness or other voice change.
The current GERD diagnostic options and treatment therapies may be inadequate, though better options are beginning to emerge. Twenty-four-hour catheter-based pH monitoring, for example, is invasive and often inconclusive as patients typically modify their activity and diet the day they wear the nasal catheter. Better but costlier options include the Bravo™ pH Monitoring System, in which a tubeless monitoring capsule is placed in the mucosal wall of the esophagus, transmitting pH data to a pager-sized receiver worn on patient’s belt over a 48-hour period; and Multichannel Intraluminal Impedance (MII) Testing, which assesses acid and non-acid reflux, adequacy of acid suppression, and symptom-reflux association. Treatment for GERD—usually aggressive acid suppression therapy, an approach that requires significant diet and lifestyle modification—may still be inadequate, and the addition of prokinetic therapy with additional medication may be necessary. Those who don’t respond sufficiently to acid suppression and prokinetic therapy may be candidates for laparoscopic Nissen fundoplication, or “antireflux surgery,” which, based on small published reports, has yielded quality of life improvements in up to 90% of patients who have undergone it.
Postinfectious or postviral cough, a harsh, dry, persistent hack remaining from an upper respiratory infection, has been historically difficult to treat. This cough creates persistent airway inflammation, which in turn causes enhanced cough sensitivity, creating a vicious cycle that inhibits healing. Postviral coughs can persist for weeks or even months and may respond to antiinflammatory agents, such as inhaled and oral steroids.
More effective cough treatment options are needed, yet no new antitussive drugs have been developed in the last half century. With the discovery of TRPV1, however, pharmaceutical companies’ interest in these medications has surged. Numerous potential novel antitussive agents are now being studied, including antagonists to eosinophil, tachykinin receptor, 5-HT receptor, and TRPV1 receptor; agonists to the delta-opioid receptor, NOP receptor, and GABA-B; endogenous cannabinoids, and large conductance Ca+2-activated K+-channel openers.
The idiopathic (unexplained) cough remains a mystery. Patients with this cough—predominantly peri-menopausal women with a lower capsaicin threshold, many of whom have had an upper respiratory infection preceding symptom onset—may have been inadequately diagnosed. However, even after aggressive, comprehensive testing and treatment, some continue to cough. A percentage of these patients are reported to have lymphocytic airway inflammation and autoimmune diseases, but the link is neither consistent nor definitive.
Chronic cough is the most common reason that patients seek medical care, yet only a fraction of people with UACS, asthma, non-asthmatic eosinophilic bronchitis, or GERD actually experience this symptom, a phenomenon yet to be understood. These individuals may possess an intrinsically hypersensitive cough reflex, more easily triggered by aggravating factors to produce the reaction.
Although cough has been historically under-researched relative to its importance as a medical problem, the last decade has witnessed a significant increase in scientific activity dedicated to understanding the mechanism of cough, and identifying more effective therapies.
 Temporary Solution
Temporary Solution