Safety Tips for Health Givers in Hospitals and Long Term Care Facilities through All American Homecare:
1 – Medical facilities such as hospitals and long-term care facilities will have people that maintain the grounds and buildings. However, as an at-home caregiver, you’ll be visiting patients’ homes that are in a variety of conditions. Be sure to watch your step while approaching the home, making sure that you don’t trip on uneven concrete and keep an eye out for rotting wood.
Once inside, do not remove your shoes, or change into a pair of shoes that you only wear indoors (it is important to keep your safety in mind while also respecting the wishes or culture of your patient). Your shoes will protect you from slipping or stubbing a toe.
Also be mindful of slippery hard surfaces, open cupboards, and other things that can cause injury when you are engrossed in helping your patient.
2 –When visiting patients, keep your guard up and be aware of your surroundings. Unlike the controlled environments of hospitals and other facilities, the homes of patients can be unpredictable.
Trust your instincts and never go into a situation that makes you feel unsafe. Be sure to call your supervisor to figure out how to proceed in these situations. Also learn to recognize warning signs and if you feel threatened, immediately leave and inform your supervisor of the situation.
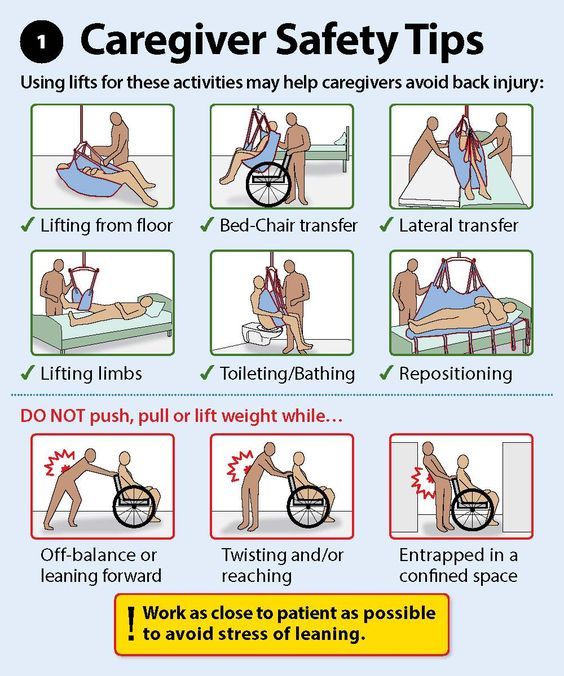
3 – It’s vital that you use safe lifting practices each time you transfer a patient. This will help reduce incidents of back injury and muscle strains. Here’s a refresher on proper lifting techniques:
- Keep your head and neck in proper alignment with your spine
- Maintain the natural curve of your spine; bend with your hips and knees, not your spine
- Avoid twisting your body when carrying the person
- Always keep the patient being moved close to your body
- Keep your feet shoulder-width apart to maintain your balance
- Use the muscles in your legs to lift and/or pull
4 – There are plenty of tools for home healthcare workers to aid them in their daily tasks. These can include lifting and transfer aides. If you are helping a patient change a light bulb, don’t stand on a chair to do it; instead, use a step stool.
5 – Your uniform (often scrubs or a pair of slacks and a polo) ensures that you are properly dressed for the job. If you don’t have a company uniform, ensure that your clothing allows you to move freely. Also, wear close-toed shoes with good traction and support.
6 – Household spills and incontinence accidents increase the risk of falls for both the caregiver and the patient. Clutter can also lead to tripping and falling. Clean up these and other safety hazards immediately.
7 – Many of your patients will have pets. Not only can animals cause you to become distracted or interfere with your work, even the friendliest pet can turn on you. Your best bet is to avoid the animals in the home and focus on your patient.
8 – One of the biggest risks to home healthcare workers is going past their limits. Make sure that you know your limits. If a patient is too heavy for you to transfer on your own, ask for help. Also, pace yourself and build flexibility into your schedule. Injury-inducing shortcuts just aren’t worth it!
Taking time to stretch throughout the day can help reduce muscle fatigue and strains. When it’s time to take a break, take it. Keep yourself hydrated throughout the day and eat a meal and snacks. Being dehydrated and not eating can lead to feelings of tiredness and making dangerous mistakes.
9 – Here are a few other basic safety protocols you need to follow:
- Confirm with your clients by phone before you visit.
- Have detailed directions to your client’s home or use a GPS device.
- Keep your vehicle in good working condition and fill up your gas tank.
- Don’t text or talk on the phone while driving.
- Keep your car doors locked and your windows closed.
- Lock your bag and other possessions in the trunk of your car.
- Most importantly, make sure that someone knows where you are at all times.
By following these safety guidelines, you’ll be able to provide better care for your patients and have a satisfying career that you enjoy each day!